



 Sign Out
Sign Out
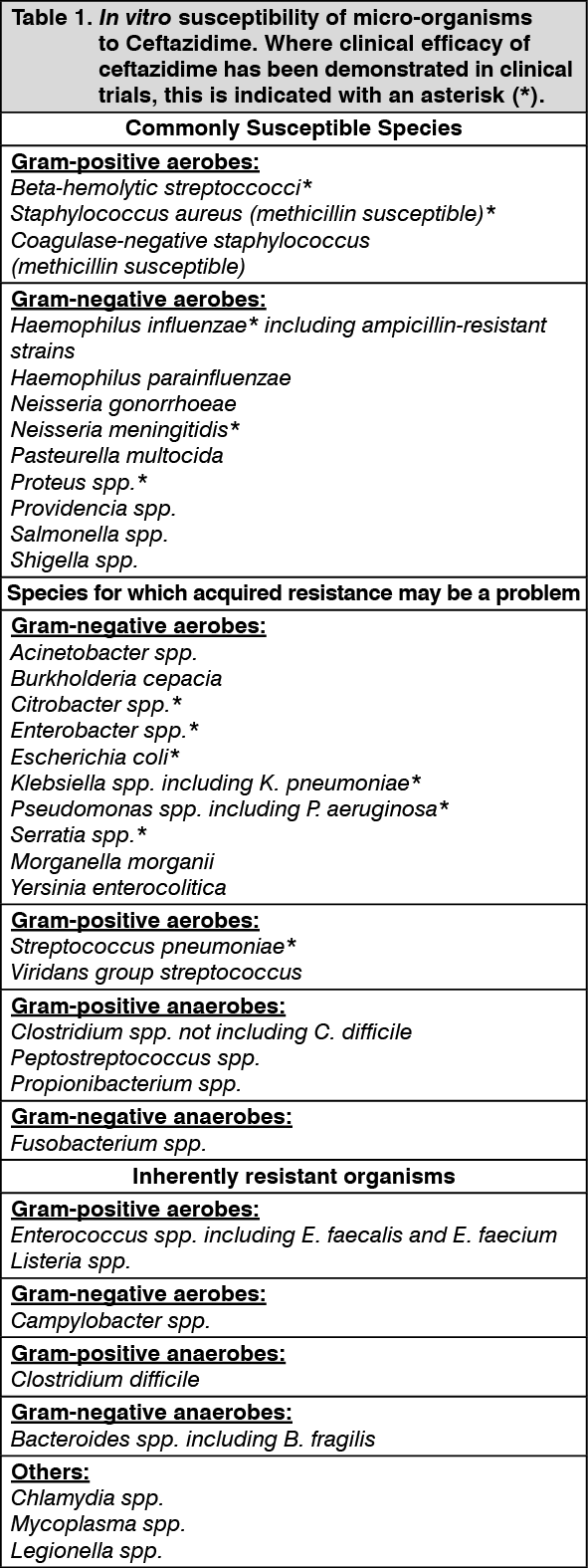
Pharmacodynamic Effects: The prevalence of acquired resistance is geographically and time dependent and for select species may be very high. Local information on resistance and prevalence of extended spectrum beta lactamase (ESBLs) producing organisms is desirable, particularly when treating severe infections. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: After i.m. administration of 500 mg and 1 g, peak levels of 18 and 37 mg/L, respectively, are achieved rapidly. Five minutes after i.v. bolus injection of 500 mg, 1 g or 2 g, serum levels are, respectively, 46, 87 and 170 mg/L.
Distribution: Therapeutically effective concentrations are still present in the serum 8 to 12 h after either i.v. or i.m. administration. Serum protein binding is about 10%. Concentrations in excess of the MIC for common pathogens can be achieved in tissues such as bone, heart, bile, sputum, aqueous humour, synovial, pleural and peritoneal fluids. Ceftazidime crosses the placenta readily, and is excreted in the breast milk. Penetration of the intact blood-brain barrier is poor resulting in low levels of ceftazidime in the CSF in the absence of inflammation. However, therapeutic levels of 4 to 20 mg/L or more are achieved in the CSF when the meninges are inflamed.
Metabolism: Ceftazidime is not metabolized in the body.
Elimination: Parenteral administration produces high and prolonged serum levels, which decrease with a half-life of about 2 h.
Ceftazidime is excreted unchanged, in active form into the urine by glomerular filtration; approximately 80 to 90% of the dose is recovered in the urine within 24 h. Less than 1% is excreted via the bile, which limits the amount entering the bowel.
Special Patient Populations: Elimination of ceftazidime is decreased in patients with impaired renal function and the dose should be reduced. (See Renal Impairment under Dosage & Administration and Precautions.)
Toxicology: Pre-clinical Safety Data: No additional data of relevance.