Tamsulosin hydrochloride.
Each prolonged release tablet contains: Tamsulosin hydrochloride, Ph.Eur. 400 mcg.
Tamsulosin hydrochloride is an antagonist of alpha1A adrenoceptors in the prostate. Tamsulosin hydrochloride is (-)-(R)-5-[2-[[2-(o-Ethoxyphenoxy) ethyl]amino]propyl]-2-methoxybenzenesulfonamide, monohydrochloride. Tamsulosin hydrochloride is a white crystalline powder that melts with decomposition at approximately 230°C. It is sparingly soluble in water and methanol, slightly soluble in glacial acetic acid and ethanol, and practically insoluble in ether.
The empirical formula of tamsulosin hydrochloride is C20H28N2O5S HCl. The molecular weight of tamsulosin hydrochloride is 444.98.
Each prolonged-release tablet contains 400 mcg tamsulosin hydrochloride, equivalent to 367 mcg tamsulosin.
Excipients/Inactive Ingredients: The following inactive ingredients: Hypromellose, Magnesium stearate, Cellulose microcrystalline, Carbomer, Silica colloidal anhydrous, Iron oxide red.
Pharmacotherapeutic group: α1A adrenoreceptor antagonist. ATC code: G04CA02.
Pharmacology: Pharmacodynamics: Mechanism of action: Tamsulosin binds selectively and competitively to the postsynaptic αI adrenoceptors, in particular to subtypes αIA and α ID. It brings about relaxation of prostatic and urethral smooth muscle.
Pharmacodynamic effects: Tamsulosin increases the maximum urinary flow rate. It relieves obstruction by relaxing smooth muscle in prostate and urethra thereby improving voiding symptoms.
It also improves the storage symptoms in which bladder instability plays an important role.
These effects on storage and voiding symptoms are maintained during long term therapy. Observational data indicate that use of tamsulosin may lead to a delay in the need for surgery or catheterization.
Alpha-blockers can reduce blood pressure by lowering peripheral resistance. No reduction in blood pressure of any clinical significance was observed during studies with tamsulosin in normotensive patients.
Pharmacokinetics: Absorption: The tamsulosin prolonged release formulation provides consistent slow release of tamsulosin, resulting in an adequate exposure, with little fluctuation over 24 hours.
Tamsulosin administered as tamsulosin prolonged release tablets is absorbed from the intestine. Of the administered dose, approximately 57% is estimated to be absorbed. A consistent slow release of tamsulosin is maintained over the whole pH range encountered in the gastro-intestinal tract with little fluctuation over 24 hours. The extent of absorption is increased by 64% and 149% (AUC and Cmax respectively) by a high fat meal compared to fasted.
The rate and extent of absorption of tamsulosin administered as tamsulosin prolonged release tablets are not affected by food.
Tamsulosin shows linear pharmacokinetics.
After a single dose of tamsulosin prolonged release formulation in the fasted state, plasma concentrations of tamsulosin peak at a median time of 6 hours. In steady state, which is reached by day 4 of multiple dosing, plasma concentrations of tamsulosin peak at 4 to 6 hours, in the fasted and fed state. Peak plasma concentrations increase from approximately 6 ng/mL after the first dose to 11 ng/mL in steady state.
As a result of the prolonged release characteristics of tamsulosin prolonged release tablets the trough concentration of tamsulosin in plasma amounts to 40% of the peak plasma concentration under fasted and fed conditions.
There is a considerable inter-patient variation in plasma levels both after single and multiple dosing.
Distribution: In man, tamsulosin is about 99% bound to plasma proteins. The volume of distribution is small (about 0.2 L/kg).
Metabolism: Tamsulosin has a low first pass effect, being metabolised slowly. Most tamsulosin is present in plasma in the form of unchanged active substance. It is metabolised in the liver.
In rats, hardly any induction of microsomal liver enzymes was seen to be caused by tamsulosin.
No dose adjustment is warranted in hepatic insufficiency.
None of the metabolites is more active than the original compound.
Excretion: Tamsulosin and its metabolites are mainly excreted in the urine. The amount excreted as unchanged active substance is estimated to be about 4 - 6% of the dose, administered as Tamsulosin prolonged release tablets.
After a single dose of Tamsulosin prolonged release tablets and in steady state, elimination half-lives of about 19 and 15 hours, respectively, have been measured.
No dose adjustment is warranted in renal impairment.
Lower urinary tract symptoms (LUTS) associated with benign prostatic hyperplasia (BPH).
Oral use.
One tablet daily.
Tamsulosin can be taken independently of food.
The tablet must be swallowed whole and not be crushed or chewed as this interferes with the prolonged release of the active substance.
No dose adjustment is warranted in renal impairment.
No dose adjustment is warranted in patients with mild to moderate hepatic insufficiency (see also Contraindications).
Paediatric population: The safety and efficacy of tamsulosin in children and adolescents have not been established. There is no relevant indication for use of tamsulosin in children.
Symptoms: Overdosage with tamsulosin hydrochloride can potentially result in severe hypotensive effects, dizziness and malaise. Severe hypotensive effects have been observed at different levels of overdosing.
Treatment: In case of acute hypotension occurring after overdose, cardiovascular support should be given. Blood pressure can be restored and heart rate brought back to normal by lying the patient down. If this does not help, then volume expanders, and when necessary, vasopressors could be employed. Renal function should be monitored and general supportive measures applied. Dialysis is unlikely to be of help, as tamsulosin is very highly bound to plasma proteins.
Measures, such as emesis, can be taken to impede absorption. When large quantities are involved, gastric lavage can be applied and activated charcoal and an osmotic laxative, such as sodium sulfate, can be administered.
Hypersensitivity to tamsulosin hydrochloride, including drug-induced angioedema or to any of the excipients.
A history of orthostatic hypotension.
Severe hepatic insufficiency.
As with other α1a adrenoceptor antagonists, a reduction in blood pressure can occur in individual cases during treatment with tamsulosin, as a result of which, rarely, syncope can occur. At the first signs of orthostatic hypotension (dizziness, weakness), the patient should sit or lie down until the symptoms have disappeared.
Before therapy with tamsulosin is initiated, the patient should be examined in order to exclude the presence of other conditions, which can cause the same symptoms as benign prostatic hyperplasia. Digital rectal examination and, when necessary, determination of prostate specific antigen (PSA) should be performed before treatment and at regular intervals afterwards. The treatment of patients with severe renal impairment (creatinine clearance of < 10 mL/min) should be approached with caution, as these patients have not been studied.
The 'Intraoperative Floppy Iris Syndrome' (IFIS, a variant of small pupil syndrome) has been observed during cataract surgery in some patients on or previously treated with tamsulosin. IFIS may lead to increased procedural complications during the operation. The initiation of therapy with tamsulosin in patients for whom cataract surgery is scheduled is not recommended. Discontinuing tamsulosin 1-2 weeks prior to cataract surgery is anecdotally considered helpful, but the benefit and duration of stopping the therapy prior to cataract surgery has not yet been established.
During pre-operative assessment, cataract surgeons and ophthalmic teams should consider whether patients scheduled for cataract surgery are being or have been treated with tamsulosin in order to ensure that appropriate measures will be in place to manage the IFIS during surgery. It is possible that a remnant of the tablet is observed in the faeces.
Tamsulosin hydrochloride should not be given in combination with strong inhibitors of CYP3A4 (e.g. ketoconazole) in patients with poor metaboliser CYP2D6 phenotype.
Tamsulosin hydrochloride should be used with caution in combination with strong (e.g. ketoconazole) and moderate (e.g. erythromycin) inhibitors of CYP3A4.
Effects on ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed. However, patients should be aware of the fact that dizziness can occur.
Not applicable, as tamsulosin is intended for male patients only.
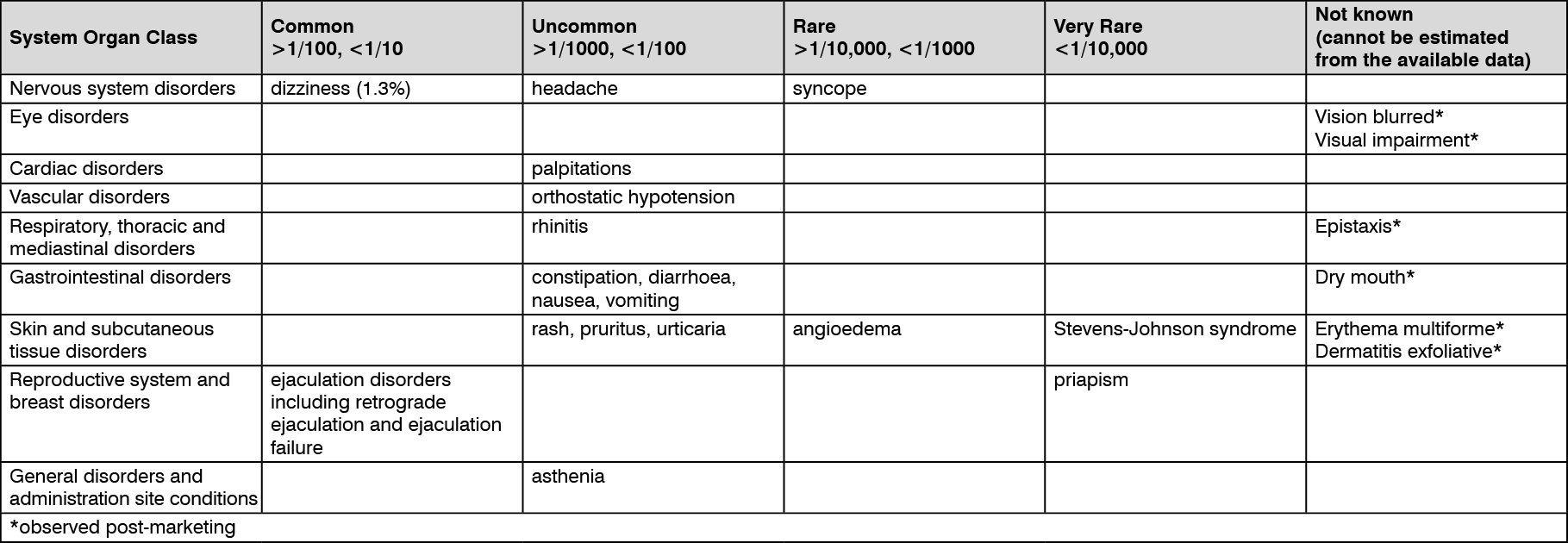
See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
As with other alpha-blockers, drowsiness, blurred vision or oedema can occur.
During cataract and glaucoma surgery a small pupil situation, known as Intraoperative Floppy Iris Syndrome (IFIS), has been associated with therapy of tamsulosin during post-marketing surveillance.
Post-marketing experience: In addition to the adverse events listed previously, atrial fibrillation, arrhythmia, tachycardia and dyspnoea have been reported in association with tamsulosin use. Because these spontaneously reported events are from the worldwide post marketing experience, the frequency of events and the role of tamsulosin in their causation cannot be reliably determined.
No interactions have been seen when tamsulosin was given concomitantly with atenolol, enalapril, or theophylline. Concomitant cimetidine brings about a rise in plasma levels of tamsulosin, and furosemide a fall, but as levels remain within the normal range, posology need not be changed.
In vitro, neither diazepam nor propranolol, trichlormethiazide, chlormadinon, amitryptyline, diclofenac, glibenclamide, simvastatin and warfarin change the free fraction of tamsulosin in human plasma. Neither does tamsulosin change the free fractions of diazepam, propranolol, trichlormethiazide, and chlormadinon.
Diclofenac and warfarin, however, may increase the elimination rate of tamsulosin.
Concomitant administration of tamsulosin hydrochloride with strong inhibitors of CYP3A4 may lead to increased exposure to tamsulosin hydrochloride. Concomitant administration with ketoconazole (a known strong CYP3A4 inhibitor) resulted in an increase in AUC and Cmax of tamsulosin hydrochloride by a factor of 2.8 and 2.2, respectively.
Tamsulosin hydrochloride should not be given in combination with strong inhibitors of CYP3A4 (e.g. ketoconazole) in patients with poor metaboliser CYP2D6 phenotype.
Tamsulosin hydrochloride should be used with caution in combination with strong (e.g. ketoconazole) and moderate inhibitors (e.g. erythromycin) of CYP3A4.
Concomitant administration of tamsulosin hydrochloride with paroxetine, a strong inhibitor of CYP2D6, resulted in a Cmax and AUC of tamsulosin that had increased by a factor of 1.3 and 1.6, respectively, but these increases are not considered clinically relevant.
There is a theoretical risk of enhanced hypotensive effect when given concurrently with drugs which may reduce blood pressure, including anaesthetic agents and other α1-adrenoceptor antagonists.
Store at temperatures not exceeding 30°C, away from direct sunlight.
G04CA02 - tamsulosin ; Belongs to the class of alpha-adrenoreceptor antagonists. Used in the treatment of benign prostatic hypertrophy.
Floezy PR tab 400 mcg
30's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out