



 Sign Out
Sign Out
Divalproex sodium/Valproate/Valproic Acid is prescribed and dispensed in accordance to the measures for prevention of pregnancy mentioned in Contraindications and Warnings.
After the treating physician determines the suitability of the patient (according to Dosage & Administration), Divalproex sodium/Valproate/Valproic Acid should preferably be prescribed as monotherapy and at the lowest effective dose, if possible as a prolonged release formulation. The daily dose should be divided into at least two single doses (see Use in Pregnancy & Lactation).
Prophylaxis of migraine attacks: Divalproex sodium/Valproate/Valproic acid should only be initiated and supervised by a specialist experienced in the management of migraine. Treatment should only be initiated if other treatments are ineffective or not tolerated (see Contraindications, Precautions and Use in Pregnancy & Lactation) and the benefit and risk should be carefully reconsidered at regular treatment reviews.
Patients with renal insufficiency: It may be necessary in patients with renal insufficiency to decrease the dosage, or to increase the dosage in patients on hemodialysis. Divalproex sodium/Valproate/Valproic acid is dialysable (see Overdosage). Dosing should be modified according to the clinical monitoring of the patient.
Valproic acid is indicated as monotherapy and adjunctive therapy in complex partial seizures in adults and pediatric patients down to the age of ten years, and in simple and complex absence seizures. As the valproic acid dosage is titrated upward, concentrations of phenobarbital, carbamazepine, and/or phenytoin may be affected (see Interactions).
Complex Partial Seizures (CPS): For adults and children ten years of age or older.
Monotherapy (Initial Therapy): Valproic acid has not been systematically studied as initial therapy. Patients should initiate therapy at 10 to 15 mg/kg/day.
The dosage should be increased by 5 to 10 mg/kg/week to achieve optimal clinical response. Ordinarily, optimal clinical response is achieved at daily doses below 60 mg/kg/day. If satisfactory clinical response has not been achieved, plasma levels should be measured to determine whether or not they are in the usually accepted therapeutic range (50 to 100 mcg/mL). No recommendation regarding the safety of valproate for use at doses above 60 mg/kg/day can be made.
The probability of thrombocytopenia increases significantly at total trough valproate plasma concentrations above 110 mcg/mL in females and 135 mcg/mL in males. The benefit of improved seizure control with higher doses should be weighed against the possibility of a greater incidence of adverse reactions (see Thrombocytopenia under Precautions).
Conversion to Monotherapy: Patients should initiate therapy at 10 to 15 mg/kg/day. The dosage should be increased by 5 to 10 mg/kg/week to achieve optimal clinical response. Ordinarily, optimal clinical response is achieved at daily doses below 60 mg/kg/day. If satisfactory clinical response has not been achieved, plasma levels should be measured to determine whether or not they are in the usually accepted therapeutic range (50 to 100 mcg/mL). No recommendation regarding the safety of valproate for use at doses above 60 mg/kg/day can be made. Concomitant antiepilepsy drug (AED) dosage can ordinarily be reduced by approximately 25% every two weeks. This reduction may be started at initiation of valproic acid therapy, or delayed by one to two weeks if there is a concern that seizures are likely to occur with a reduction. The speed and duration of withdrawal of the concomitant AED can be highly variable, and patients should be monitored closely during this period for increased seizure frequency.
Adjunctive Therapy: Valproic acid may be added to the patient's regimen at a dosage of 10 to 15 mg/kg/day. The dosage may be increased by 5 to 10 mg/kg/week to achieve optimal clinical response. Ordinarily, optimal clinical response is achieved at daily doses below 60 mg/kg/day. If satisfactory clinical response has not been achieved, plasma levels should be measured to determine whether or not they are in the usually accepted therapeutic range (50 to 100 mcg/mL). No recommendation regarding the safety of valproate for use at doses above 60 mg/kg/day can be made. If the total daily dose exceeds 250 mg, it should be given in divided doses.
In a study of adjunctive therapy for complex partial seizures in which patients were receiving either carbamazepine or phenytoin in addition to divalproex sodium, no adjustment of carbamazepine or phenytoin dosage was needed (see Pharmacology: Pharmacodynamics: Clinical Studies under Actions). However, since valproate may interact with these or other concurrently administered AEDs as well as other drugs, periodic plasma concentration determinations of concomitant AEDs are recommended during the early course of therapy (see Interactions).
Simple and Complex Absence Seizures: The recommended initial dose is 15 mg/kg/day, increasing at one week intervals by 5 to 10 mg/kg/day until seizures are controlled or side effects preclude further increases. The maximum recommended dosage is 60 mg/kg/day. If the total daily dose exceeds 250 mg, it should be given in divided doses.
A good correlation has not been established between daily dose, serum concentrations, and therapeutic effect. However, therapeutic valproate serum concentrations for most patients with absence seizures will range from 50 to 100 mcg/mL. Some patients may be controlled with lower or higher serum concentrations (see Pharmacology: Pharmacodynamics: Clinical Studies under Actions).
As the valproic acid dosage is titrated upward, blood concentrations of phenobarbital and/or phenytoin may be affected (see Interactions).
Antiepilepsy drugs should not be abruptly discontinued in patients in whom the drug is administered to prevent major seizures because of the strong possibility of precipitating status epilepticus with attendant hypoxia and threat to life.
Table 3 is a guide for the initial daily dose of Valproic acid (15 mg/kg/day): See Table 3.
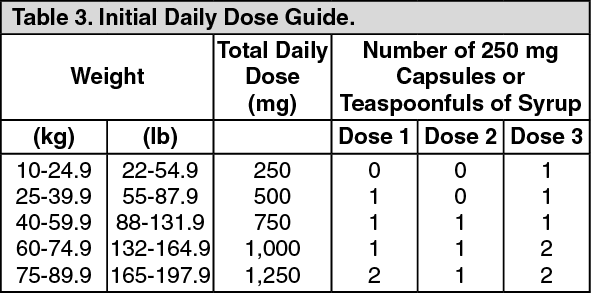 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageConversion from Valproic Acid to Divalproex Sodium: In patients previously receiving valproic acid (Depakene) therapy, divalproex sodium (Depakote) products should be initiated at the same daily dose and dosing schedule. After the patient is stabilized on a divalproex sodium product, a dosing schedule of two or three times a day may be elected in selected patients.
Female children, female adolescents, women of childbearing potential and pregnant women Divalproex sodium should be initiated and supervised by a specialist experienced in the management of epilepsy.
Treatment should only be initiated if other treatments are ineffective or not tolerated and the benefit and risk should be carefully reconsidered at regular treatment reviews. Preferably divalproex sodium should be prescribed as monotherapy and at the lowest effective dose, if possible as a prolonged release formulation to avoid high peak plasma concentrations. The daily dose should be divided into at least two single doses.
General Dosing Advice: Geriatric: Due to a decrease in clearance of unbound valproate and possibly a greater sensitivity to somnolence in the elderly, the starting dose should be reduced in these patients. Dosage should be increased more slowly and with regular monitoring for fluid and nutritional intake, dehydration, somnolence, and other adverse events. Dose reductions or discontinuation of valproate should be considered in patients with decreased food or fluid intake and in patients with excessive somnolence. The ultimate therapeutic dose should be achieved on the basis of both tolerability and clinical response (see Somnolence in the Elderly under Precautions and Pharmacology: Pharmacokinetics: Special Population: Geriatric under Actions).
Dose-Related Adverse Events: The frequency of adverse effects (particularly elevated liver enzymes and thrombocytopenia) may be dose-related. The probability of thrombocytopenia appears to increase significantly at total valproate concentrations of ≥110 mcg/mL (females) or ≥135 mcg/mL (males) (see Thrombocytopenia under Precautions). The benefit of improved therapeutic effect with higher doses should be weighed against the possibility of a greater incidence of adverse reactions.
Valproic acid capsules, syrup and tablets are antiepileptics for oral administration.
G.I. Irritation: Patients who experience G.I. irritation may benefit from administration of the drug with food or by slowly building up the dose from an initial low level.