Clinical Studies Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Most Commonly Occurring Adverse Reactions: neutropenia, thrombocytopenia, anemia, fatigue, pyrexia, nausea, cough, petechiae, constipation, diarrhea, and hyperglycemia.
Adverse Reactions Most Frequently (≥1%) Resulting in Clinical Intervention in the Phase 3 Trials in the Decitabine for Injection Arm: Discontinuation: thrombocytopenia, neutropenia, pneumonia,
Mycobacterium avium complex infection, cardio-respiratory arrest, increased blood bilirubin, intracranial hemorrhage, abnormal liver function tests.
Dose Delayed: neutropenia, pulmonary edema, atrial fibrillation, central line infection, febrile neutropenia.
Dose Reduced: neutropenia, thrombocytopenia, anemia, lethargy, edema, tachycardia, depression, pharyngitis.
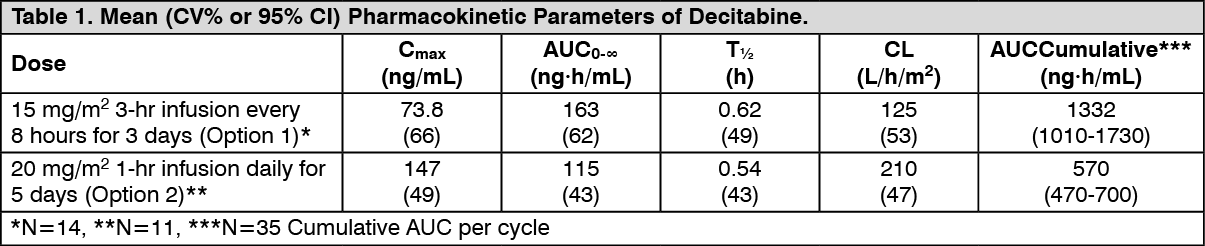
Discussion of Adverse Reactions Information: Decitabine for Injection was studied in 3 single-arm studies (N=66, N=98, N=99) and 1 controlled supportive care study (N=83 Decitabine for Injection, N=81 supportive care). The data described as follows reflect exposure to Decitabine for Injection in 83 patients in the MDS trial. In the trial, patients received 15 mg/m
2 intravenously every 8 hours for 3 days every 6 weeks. The median number of Decitabine for Injection cycles was 3 (range 0 to 9).
Tables 2a and 2b present all adverse events regardless of causality occurring in at least 5% of patients in the Decitabine for Injection group and at a rate greater than supportive care. (See Tables 2a, 2b, 3a and 3b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Serious Adverse Events that occurred in patients receiving Decitabine for Injection regardless of causality, not previously reported in Tables 2a, 2b, 3a and 3b include:
Blood and Lymphatic System Disorders: myelosuppression, splenomegaly.
Cardiac Disorders: myocardial infarction, cardio-respiratory arrest, cardiomyopathy, atrial fibrillation, supraventricular tachycardia.
Gastrointestinal Disorders: gingival pain, upper gastrointestinal hemorrhage.
General Disorders and Administrative Site Conditions: chest pain, catheter site hemorrhage.
Hepatobiliary Disorders: cholecystitis.
Infections and Infestations: fungal infection, sepsis, bronchopulmonary aspergillosis, peridiverticular abscess, respiratory tract infection, pseudomonal lung infection,
Mycobacterium avium complex infection.
Injury, Poisoning and Procedural Complications: post procedural pain, post procedural hemorrhage.
Nervous System Disorders: intracranial hemorrhage.
Psychiatric Disorders: mental status changes.
Renal and Urinary Disorders: renal failure, urethral hemorrhage.
Respiratory, Thoracic and Mediastinal Disorders: hemoptysis, lung infiltration, pulmonary embolism, respiratory arrest, pulmonary mass.
Allergic Reaction: Hypersensitivity (anaphylactic reaction) to Decitabine for Injection has been reported in a Phase 2 trial.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image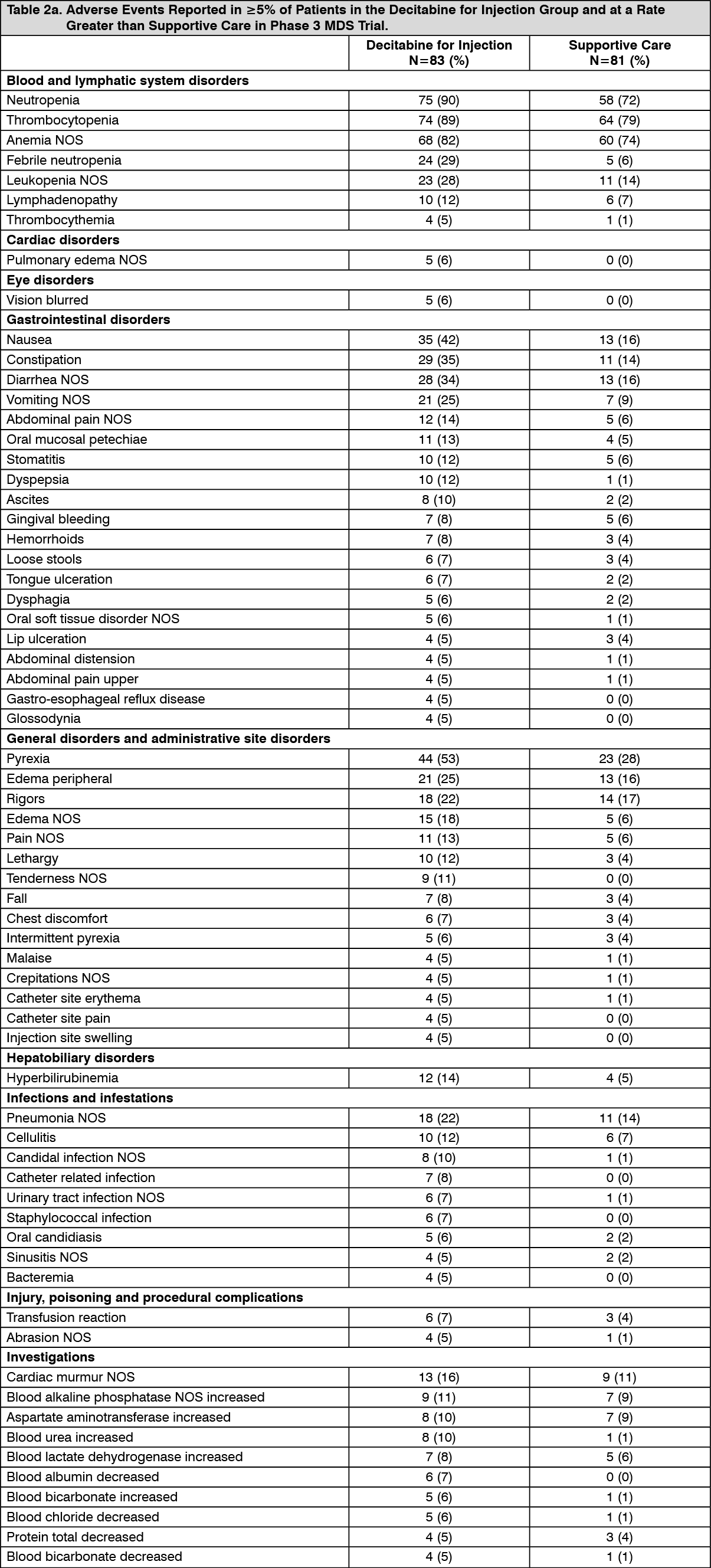 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image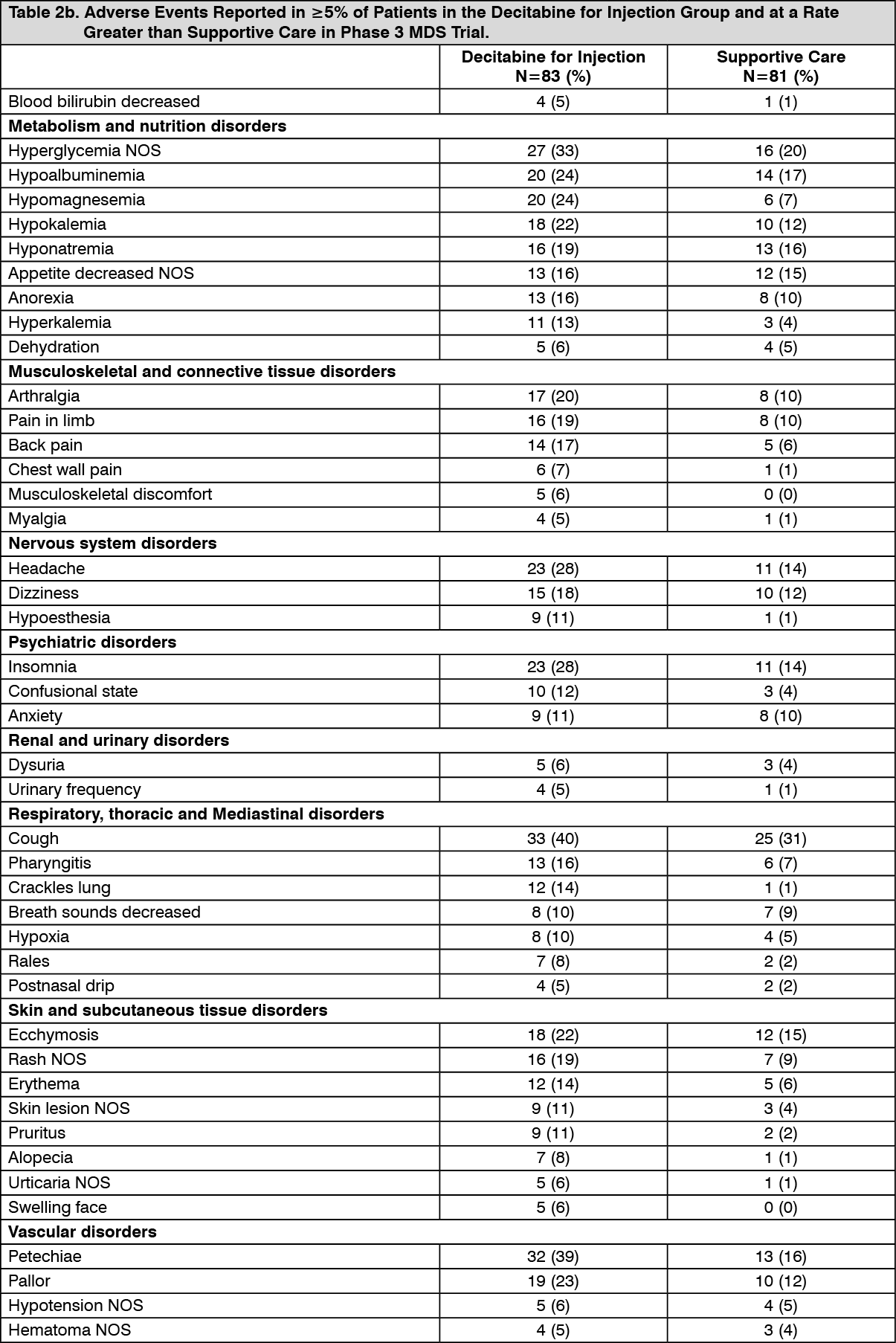 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image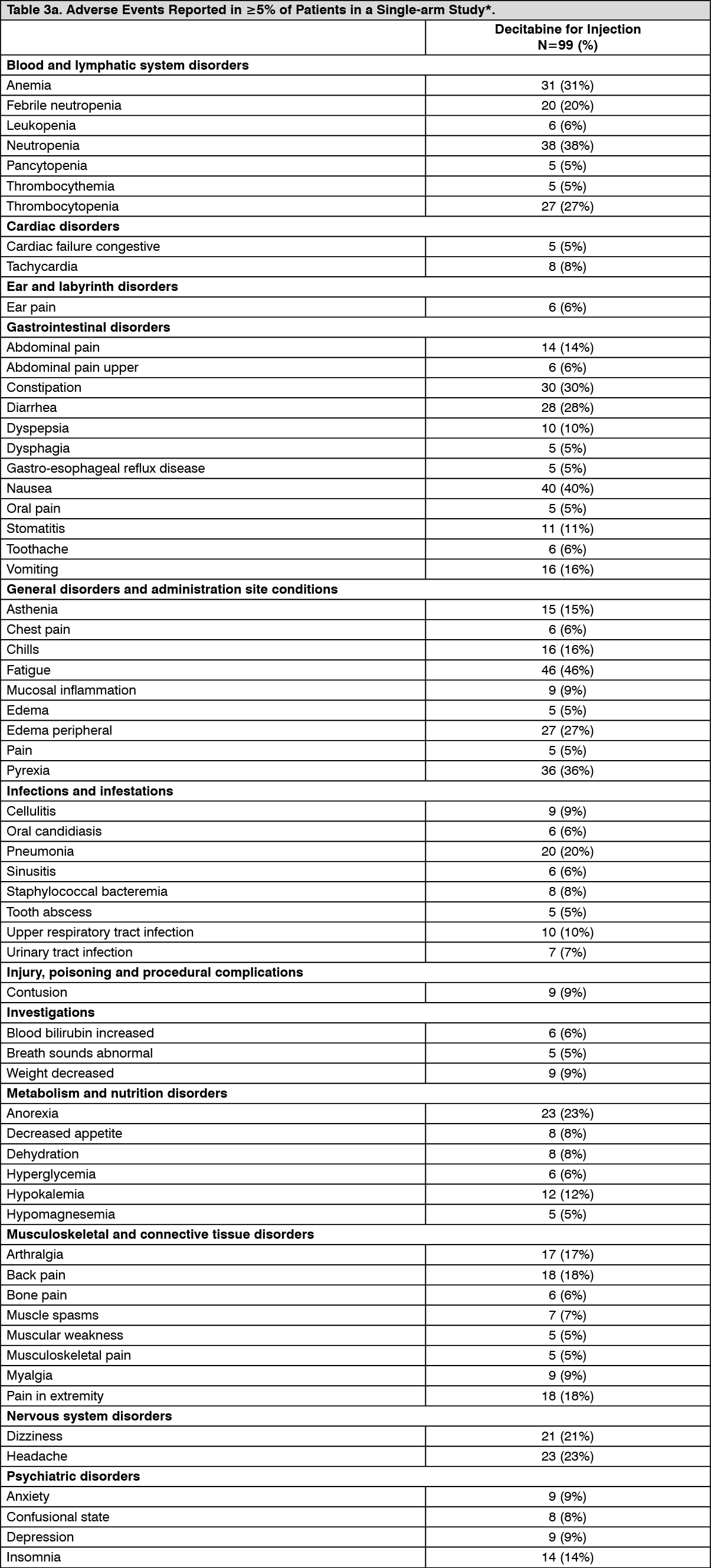 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image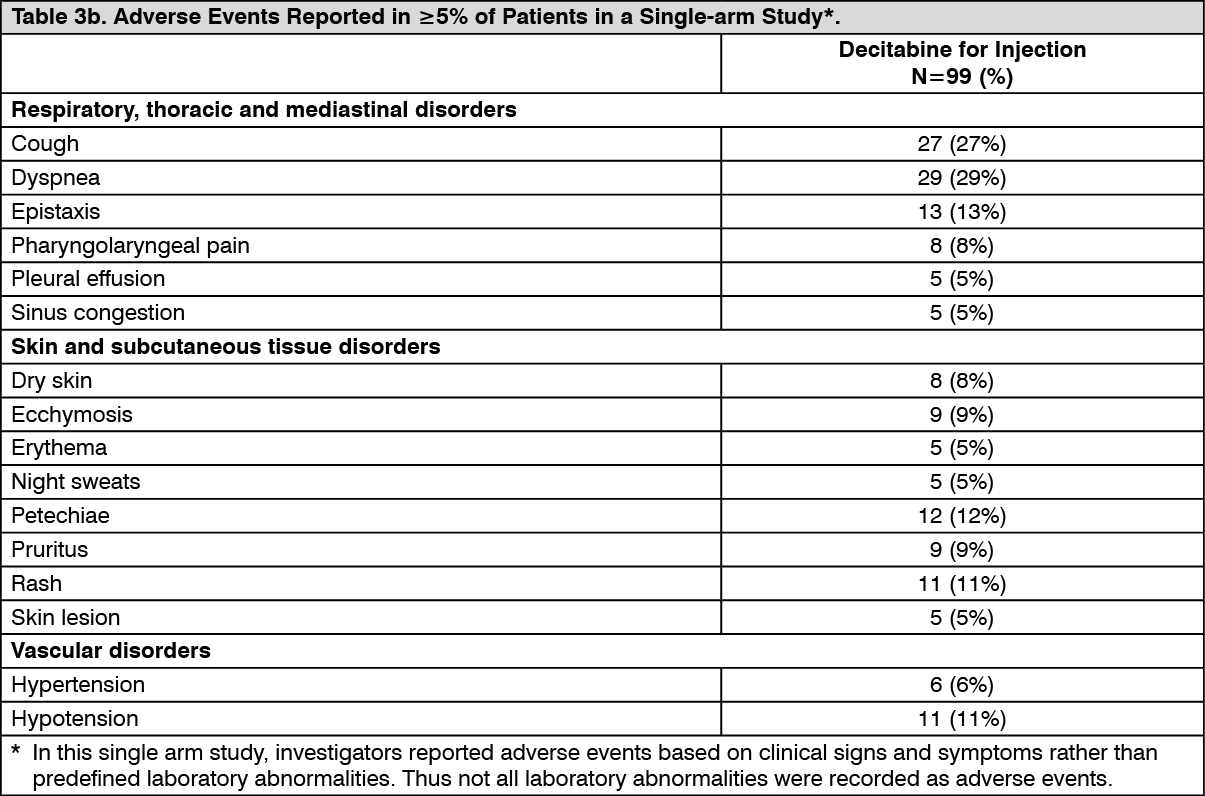 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out