Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. Dapagliflozin has been evaluated in clinical trials in patients with type 2 diabetes mellitus. The overall safety profile of Dapagliflozin was consistent across the studied indications. Severe hypoglycemia and Diabetic ketoacidosis (DKA) were observed only in patients with diabetes mellitus.
Clinical Trials in Patients with Type 2 Diabetes Mellitus: Table 2 shows common adverse reactions in published placebo-controlled studies of glycemic control reported in ≥2% of patients treated with Dapagliflozin. These adverse reactions were not present at baseline, occurred more commonly on Dapagliflozin than on placebo, and occurred in at least 2% of patients treated with either Dapagliflozin 5 mg or Dapagliflozin 10 mg. (See Table 2.)
 Click on icon to see table/diagram/image
Volume Depletion:
Click on icon to see table/diagram/image
Volume Depletion: Dapagliflozin causes an osmotic diuresis, which may lead to a reduction in intravascular volume. Adverse reactions related to volume depletion (including reports of dehydration, hypovolemia, orthostatic hypotension, or hypotension) in patients with type 2 diabetes mellitus.
Hypoglycemia: The frequency of hypoglycemia by study in patients with type 2 diabetes mellitus is shown in table 3. Hypoglycemia was more frequent when Dapagliflozin was added to sulfonylurea or insulin. (See Table 3.)
Click on icon to see table/diagram/image
Genital Mycotic Infections: The most frequently reported genital mycotic infections were vulvovaginal mycotic infections in females and balanitis in males. Patients with a history of genital mycotic infections were more likely to have a genital mycotic infection during the study than those with no prior history (10.0%, 23.1%, and 25.0% versus 0.8%, 5.9%, and 5.0% on placebo, Dapagliflozin 5 mg, and Dapagliflozin 10 mg, respectively).
Hypersensitivity Reactions: Hypersensitivity reactions (e.g., angioedema, urticaria and hypersensitivity) were reported with Dapagliflozin treatment.
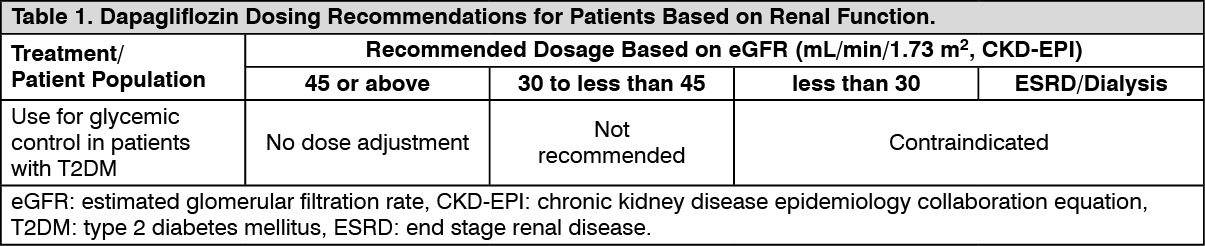
Laboratory Tests: Increases in Serum Creatinine and Decreases in eGFR: Initiation of SGLT2 inhibitors, including Dapagliflozin causes a small increase in serum creatinine and decrease in eGFR. In patients with normal or mildly impaired renal function at baseline, these changes in serum creatinine and eGFR generally occur within weeks of starting therapy and then stabilize. Increases that do not fit this pattern should prompt further evaluation to exclude the possibility of acute kidney injury. The acute effect on eGFR reverses after treatment discontinuation, suggesting acute hemodynamic changes may play a role in the renal function changes observed with Dapagliflozin.
Increase in Hematocrit: In the pool of 13 published placebo-controlled studies of glycemic control, increases from baseline in mean hematocrit values were observed in Dapagliflozin-treated patients starting at week 1 and continuing up to week 16, when the maximum mean difference from baseline was observed. At week 24, the mean changes from baseline in hematocrit were -0.33% in the placebo group and 2.30% in the Dapagliflozin 10 mg group. By week 24, hematocrit values >55% were reported in 0.4% of placebo-treated patients and 1.3% of Dapagliflozin 10 mg-treated patients.
Decrease in Serum Bicarbonate: In a published study of concomitant therapy of Dapagliflozin 10 mg with exenatide extended-release (on a background of metformin), four patients (1.7%) on concomitant therapy had a serum bicarbonate value of less than or equal to 13 meq/L compared to one each (0.4%) in the Dapagliflozin and exenatide extended-release treatment groups.
Seek medical attention immediately at the first sign of any adverse drug reaction.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image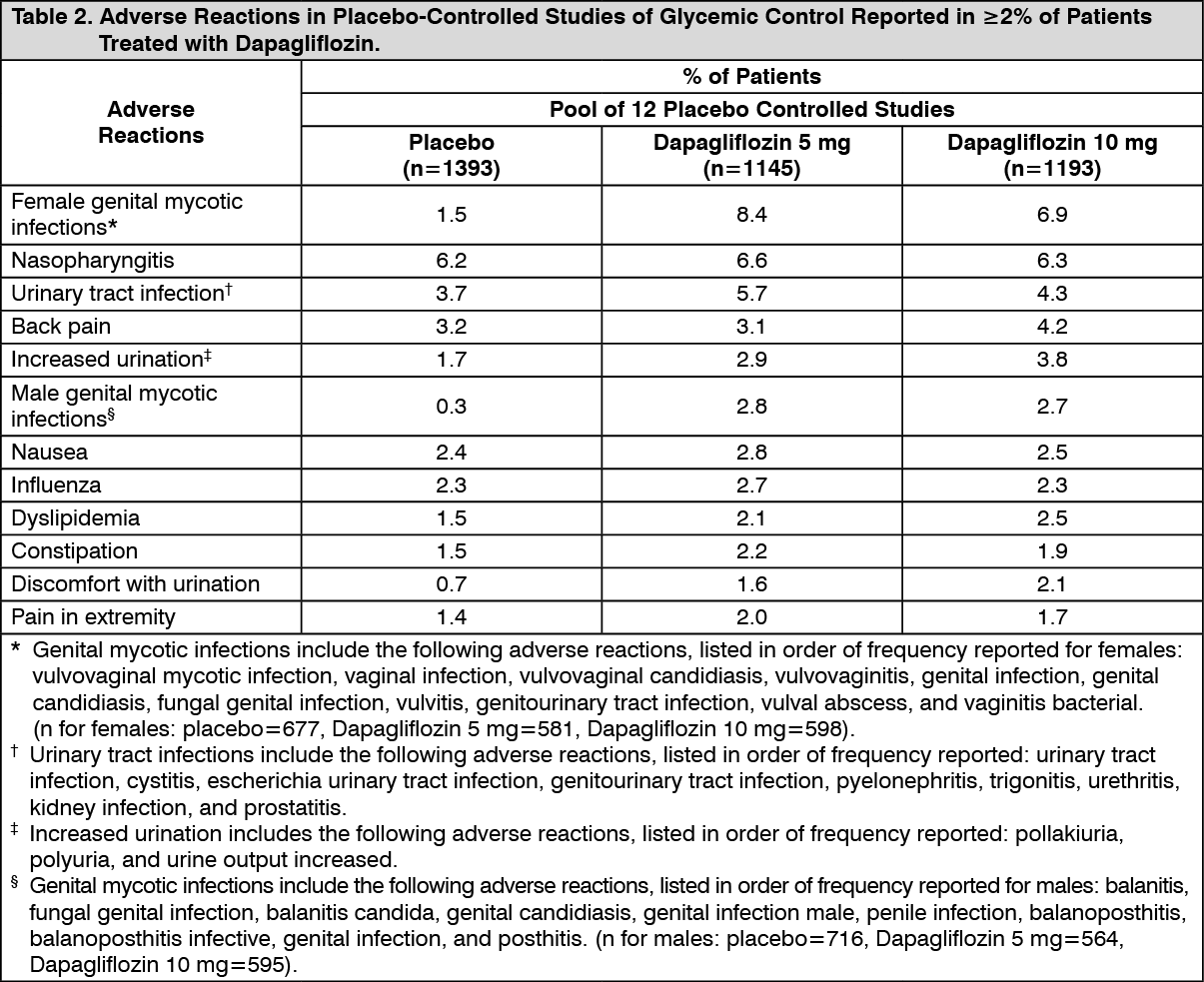 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image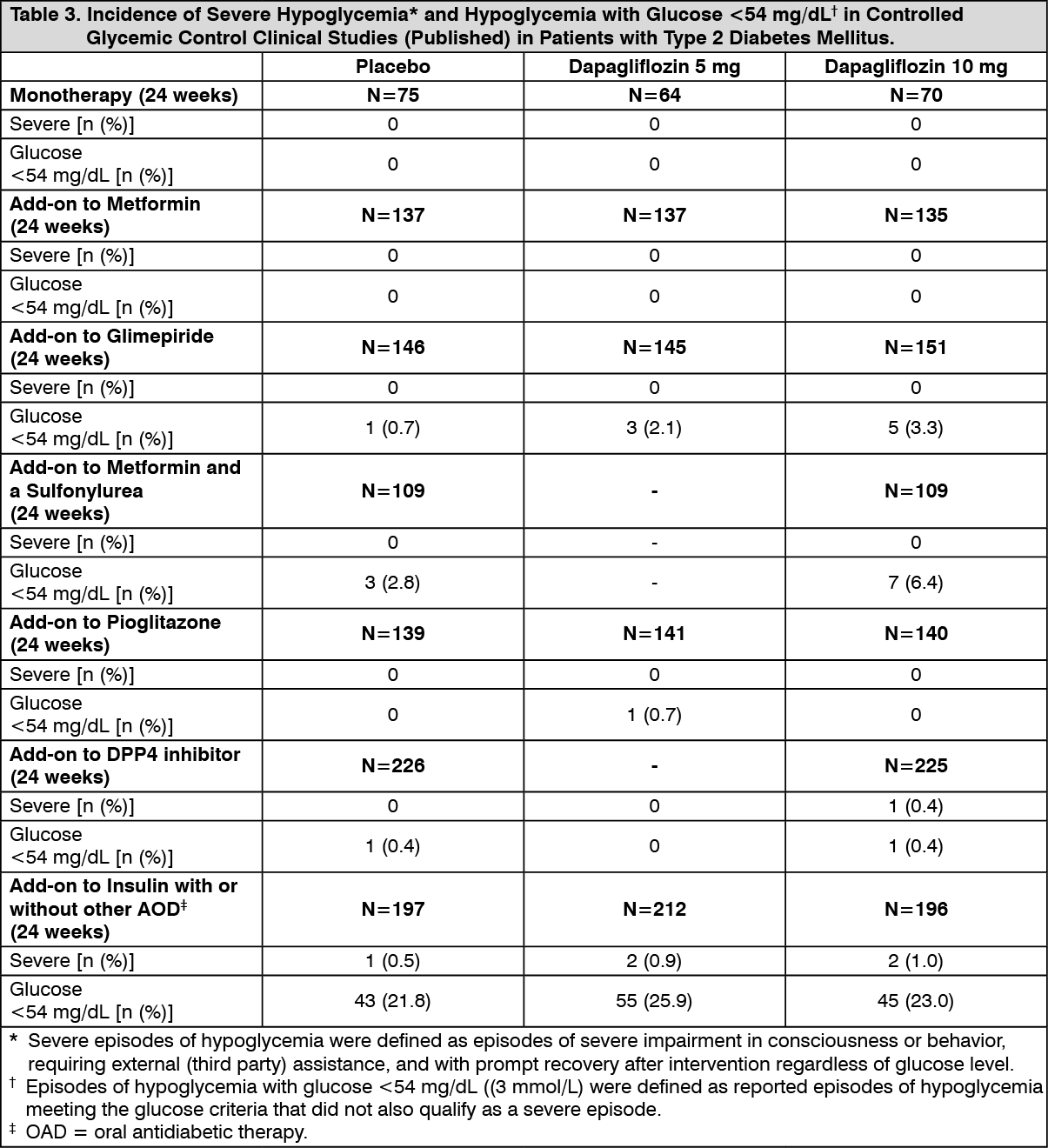 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out