Therapeutic/Pharmacologic Class of the Drug: Anticytomegalovirus.
ATC code: J05AB06.
Pharmacology: Pharmacodynamics: Mechanism of Action: Ganciclovir is a synthetic analogue of 2'-deoxyguanosine which inhibits replication of herpes viruses
in vitro, and
in vivo. Sensitive human viruses include human cytomegalovirus (HCMV), herpes-simplex virus-1 and -2 (HSV-1 and HSV-2), human herpes virus -6, -7 and -8 (HHV-6, HHV-7, HHV-8), Epstein-Barr virus (EBV), varicella-zoster virus (VZV) and hepatitis B virus. However, clinical studies have been limited to assessment of efficacy in patients with CMV infection. In CMV infected cells, ganciclovir is initially phosphorylated to ganciclovir monophosphate by the viral protein kinase, UL97. Further phosphorylation occurs by several cellular kinases to produce ganciclovir triphosphate, which is then slowly metabolized intracellularly. This has been shown to occur in HSV- and HCMV-infected cells with half-lives of 18 and between 6 and 24 hours respectively after removal of extracellular ganciclovir. As the phosphorylation is largely dependent on the viral kinase, phosphorylation of ganciclovir occurs preferentially in virus-infected cells.
The virustatic activity of ganciclovir is due to the inhibition of viral DNA synthesis by: competitive inhibition of incorporation of deoxyguanosine triphosphate into DNA by DNA polymerase; and incorporation of ganciclovir triphosphate into viral DNA causing termination of, or very limited, viral DNA elongation. Typical anti-viral IC
50 against CMV
in vitro is in the range 0.08 μM (0.02 μg/mL) to 14 μM (3.5 μg/mL).
Clinical/Efficacy Studies: No text on clinical studies.
Viral resistance: Viruses resistant to ganciclovir can arise after chronic dosing with ganciclovir or valganciclovir by selection of mutations in either the viral kinase gene (UL97) responsible for ganciclovir monophosphorylation or the viral polymerase gene (UL54). UL97 mutations arise earlier and more frequently than mutations in UL54. Virus containing mutations in the UL97 gene is resistant to ganciclovir alone, with M460V/I, H520Q, C592G, A594V, L595S, C603W being the most frequently reported ganciclovir resistance-associated substitutions. Mutations in the UL54 gene may show cross-resistance to other antivirals targeting the viral polymerase, and vice versa. Amino acid substitutions in UL54 conferring cross-resistance to ganciclovir and cidofovir are generally located within the exonuclease domains and region V, however amino acid substitutions conferring cross-resistance to foscarnet are diverse, but concentrate at and between regions II (codon 696-742) and III (codon 805-845).
The possibility of viral resistance should be considered in patients who repeatedly achieve a poor clinical response or experience continuous viral excretion during treatment.
Immunogenicity: Not applicable.
Pharmacokinetics: The pharmacokinetics of IV ganciclovir is linear over the range of 1.6-5.0 mg/kg. The systemic exposure (AUC
0-∞) reported following dosing with a single 1-hour IV infusion of 5 mg/kg ganciclovir in adult liver transplant patients was on average 50.6 μg.h/mL (CV% 40). In this patient population, peak plasma concentration (C
max) was on average 12.2 μg/mL (CV% 24).
Absorption: Not applicable.
Distribution: For IV ganciclovir, the volume of distribution is correlated with body weight with values for the steady state volume of distribution ranging from 0.54 to 0.87 L/kg. Ganciclovir penetrates the cerebrospinal fluid, and diffuses across the placenta. Binding to plasma proteins was 1%-2% over ganciclovir concentrations of 0.5 and 51 μg/mL.
Metabolism: Ganciclovir is not metabolized to a significant extent.
Elimination: Renal excretion of unchanged drug by glomerular filtration and active tubular secretion is the major route of elimination of ganciclovir. In patients with normal renal function, greater than 90% of IV administered ganciclovir was recovered unmetabolized in the urine within 24 hours.
In patients with normal renal function, systemic clearance ranged from 2.64 ± 0.38 mL/min/kg (N=15) to 4.52 ± 2.79 mL/min/kg (N=6) and renal clearance ranged from 2.57 ± 0.69 mL/min/kg (N=15) to 3.48 ± 0.68 mL/min/kg (N=20), corresponding to 90%-101% of administered ganciclovir. Half-lives in patients without renal impairment ranged from 2.73 ± 1.29 (N=6) to 3.98 ± 1.78 hours (N=8).
Pharmacokinetics in Special Populations: Pediatric population: The pharmacokinetics of IV ganciclovir were investigated across two studies in pediatric liver (N=18) and renal (N=25) transplant patients aged 3 months to 16 years and evaluated using a population pharmacokinetic model. The mean total clearance was 5.4 L/hr (90 mL/min) for a child with a creatinine clearance of 70.4 mL/min. The steady state volume of distribution and peripheral volume of distribution were on average 20 and 15 L, respectively. CrCL was identified as statistically significant covariate for ganciclovir clearance and height of the patient as statistically significant covariate for ganciclovir clearance, steady state volume and peripheral volume of distribution. Neither age, gender, nor types of organ transplant were significant covariates in these populations. Table 1 gives the estimated pharmacokinetic parameters by age group. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics of IV ganciclovir given according to the dosing regimen approved for adults (5 mg/kg IV infusion administered over 1 hour) were studied in a small group of infants and children with normal renal function, aged 9 months to 12 years (n=10, average 3.1 years). Exposure as measured by mean AUC
∞ on Day 1 (n=10) and AUC
0-12h on Day 14 (n=7) were 19.4 ± 7.1 and 24.1 ± 14.6 μg.h/mL with 0-12 corresponding C
max values of 7.59 ± 3.21 and 8.31 ± 4.9 μg/mL (Days 1 and 14) respectively. A trend towards lower exposures in younger pediatric patients was observed with body weight based dosing used in this study. In pediatric patients up to 5 years the average values for AUC
0-∞ on Day 1 (n=7) and AUC
0-12h on Day 14 (n=4) were 17.7 ± 5.5 and 17.1 ± 7.5 μg.h/mL.
The ganciclovir IV dosing regimen based on BSA and renal function (3x BSA x CrCLS) is derived from the pediatric dosing algorithm with valganciclovir, the oral pro-drug of ganciclovir. Pharmacokinetic simulations have confirmed that both dosing regimens provide similar ganciclovir exposures in the pediatric population from birth to 16 years. (See Table 2.)
Click on icon to see table/diagram/image
Geriatric population: No ganciclovir pharmacokinetic studies have been conducted in adults older than 65 years of age. However, because ganciclovir is mainly renally excreted and since renal clearance decreases with age a decrease in ganciclovir total body clearance and prolongation of ganciclovir elimination half-life can be anticipated in the elderly (see Special Dosage Instructions: Geriatric patients under Dosage & Administration).
Renal impairment: The total body clearance of ganciclovir is linearly correlated with creatinine clearance. In patients with mild, moderate, and severe renal impairment, mean systemic clearances of 2.1, 1.0 and 0.3 mL/min/kg were observed. Patients with renal impairment show an increased elimination half-life. In patients with severe renal impairment elimination half-life was increased by 10-fold (see Special Dosage Instructions: Renal impairment under Dosage & Administration).
Patients undergoing hemodialysis: Plasma concentrations of ganciclovir are reduced by about 50% during a 4 hour hemodialysis session (see Overdosage).
During intermittent hemodialysis, estimates for the clearance of ganciclovir ranged from 42 to 92 mL/min, resulting in intra-dialytic half-lives of 3.3 to 4.5 hours.
Estimates of ganciclovir clearance for continuous dialysis were lower (4.0 to 29.6 mL/min) but resulted in greater removal of ganciclovir over a dose interval. For intermittent hemodialysis, the fraction of ganciclovir removed in a single dialysis session varied from 50% to 63%.
Hepatic impairment: No pharmacokinetic study has been conducted and no population PK data were collected in patients with hepatic impairment undergoing ganciclovir therapy. Hepatic impairment is not anticipated to affect the pharmacokinetics of ganciclovir since ganciclovir is excreted renally (see Elimination as previously mentioned).
Toxicology: Nonclinical Safety: Carcinogenicity: Ganciclovir was mutagenic in mouse lymphoma cells and clastogenic in mammalian cells. Such results are consistent with the positive mouse carcinogenicity study with ganciclovir. Ganciclovir is a potential carcinogen.
Genotoxicity: Ganciclovir was mutagenic in mouse lymphoma cells and clastogenic in mammalian cells.
Impairment of Fertility: Ganciclovir causes impaired fertility and teratogenicity in animals (see Precautions).
Based upon animal studies where aspermia was induced at ganciclovir systemic exposures below therapeutic levels, it is considered likely that ganciclovir could cause temporary or permanent inhibition of human spermatogenesis (see Females and Males of Reproductive Potential: Fertility under Use in Pregnancy & Lactation).
Reproductive toxicity: Ganciclovir causes teratogenicity in animals.
Other: No additional information is available.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image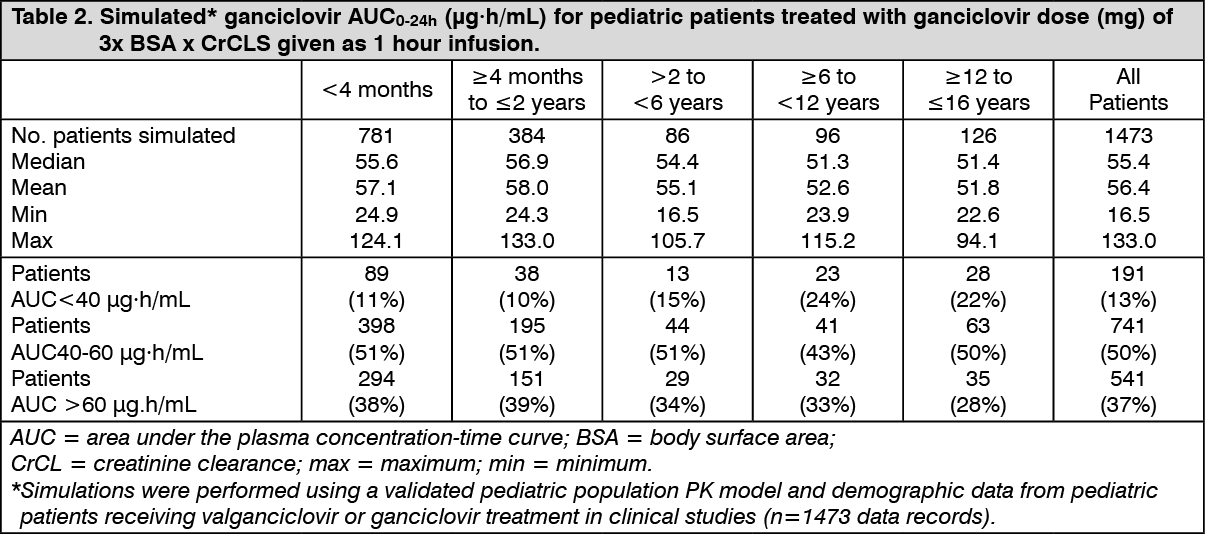 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out