Co-amoxiclav: Amoxicillin, clavulanic acid.
White to off white coloured, elliptical, biconvex film-coated tablet.
Each film-coated tablet contains: Amoxicillin Trihydrate eq. to Amoxicillin USP 500 mg; Clavulanate potassium eq. to Clavulanic acid 125 mg.
Pharmacotherapeutic group: Combinations of penicillins, including beta-lactamase inhibitors.
Pharmacology: Pharmacodynamics: Mechanism of action: Amoxicillin is a semisynthetic penicillin (beta-lactam antibiotic) that inhibits one or more enzymes (often referred to as penicillin-binding proteins, PBPs) in the biosynthetic pathway of bacterial peptidoglycan, which is an integral structural component of the bacterial cell wall. Inhibition of peptidoglycan synthesis leads to weakening of the cell wall, which is usually followed by cell lysis and death.
Amoxicillin is susceptible to degradation by beta-lactamases produced by resistant bacteria and therefore the spectrum of activity of amoxicillin alone does not include organisms which produce these enzymes.
Clavulanic acid is a beta-lactam structurally related to penicillins. It inactivates some beta-lactamase enzymes thereby preventing inactivation of amoxicillin. Clavulanic acid alone does not exert a clinically useful antibacterial effect.
Pharmacokinetics: Absorption: Amoxicillin and clavulanic acid, are fully dissociated in aqueous solution at physiological pH. Both components are rapidly and well absorbed by the oral route of administration. Following oral administration, amoxicillin and clavulanic acid are approximately 70% bioavailable. The plasma profiles of both components are similar and the time to peak plasma concentration (Tmax) in each case is approximately one hour.
Distribution: About 25% of total plasma clavulanic acid and 18% of total plasma amoxicillin is bound to protein. The apparent volume of distribution is around 0.3-0.4 l/kg for amoxicillin and around 0.2 l/kg for clavulanic acid.
Following intravenous administration, both amoxicillin and clavulanic acid have been found in gall bladder, abdominal tissue, skin, fat, muscle tissues, synovial and peritoneal fluids, bile and pus. Amoxicillin does not adequately distribute into the cerebrospinal fluid.
From animal studies there is no evidence for significant tissue retention of drug-derived material for either component.
Amoxicillin, like most penicillins, can be detected in breast milk. Trace quantities of clavulanic acid can also be detected in breast milk.
Both amoxicillin and clavulanic acid have been shown to cross the placental barrier.
Biotransformation: Amoxicillin is partly excreted in the urine as the inactive penicilloic acid in quantities equivalent to up to 10 to 25% of the initial dose. Clavulanic acid is extensively metabolized in man and eliminated in urine and faeces, and as carbon dioxide in expired air.
Elimination: The major route of elimination for amoxicillin is via the kidney, whereas for clavulanic acid it is by both renal and non-renal mechanisms.
Amoxicillin/clavulanic acid has a mean elimination half-life of approximately one hour and a mean total clearance of approximately 25 l/h in healthy subjects. Approximately 60 to 70% of the amoxicillin and approximately 40 to 65% of the clavulanic acid are excreted unchanged in urine during the first 6 h after administration of single Augmentin 250 mg/125 mg or 500 mg/125 mg tablets. Various studies have found the urinary excretion to be 50-85% for amoxicillin and between 27-60% for clavulanic acid over a 24 hour period. In the case of clavulanic acid, the largest amount of drug is excreted during the first 2 hours after administration.
Concomitant use of probenecid delays amoxicillin excretion but does not delay renal excretion of clavulanic acid.
Age: The elimination half-life of amoxicillin is similar for children aged around 3 months to 2 years and older children and adults. For very young children (including preterm newborns) in the first week of life the interval of administration should not exceed twice daily administration due to immaturity of the renal pathway of elimination. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Gender: Following oral administration of amoxicillin/clavulanic acid to healthy males and female subjects, gender has no significant impact on the pharmacokinetics of either amoxicillin or clavulanic acid.
Renal impairment: The total serum clearance of amoxicillin/clavulanic acid decreases proportionately with decreasing renal function. The reduction in drug clearance is more pronounced for amoxicillin than for clavulanic acid, as a higher proportion of amoxicillin is excreted via the renal route. Doses in renal impairment must therefore prevent undue accumulation of amoxicillin while maintaining adequate levels of clavulanic acid.
Hepatic impairment: Hepatically impaired patients should be dosed with caution and hepatic function monitored at regular intervals.
Amoxicillin with Clavulanic acid is indicated for the treatment of the following infections in adults and children: Acute bacterial sinusitis (adequately diagnosed), Acute otitis media, Acute exacerbations of chronic bronchitis (adequately diagnosed), Community acquired pneumonia, Cystitis, Pyelonephritis, Skin and soft tissue infections in particular cellulitis, animal bites, severe dental abscess with spreading cellulitis, Bone and joint infections, in particular osteomyelitis.
For adults and children ≥40 kg, this formulation of Co-Amoxiclav provides a total daily dose of 1500 mg amoxicillin/375 mg clavulanic acid, when administered as recommended as follows. For children <40 kg, this formulation of Co-Amoxiclav provides a maximum daily dose of 2400 mg amoxicillin/600 mg clavulanic acid, when administered as recommended as follows. If it is considered that a higher daily dose of amoxicillin is required, it is recommended that another preparation of Co-Amoxiclav is selected in order to avoid administration of unnecessarily high daily doses of clavulanic acid.
The duration of therapy should be determined by the response of the patient. Some infections (e.g. osteomyelitis) require longer periods of treatment. Treatment should not be extended beyond 14 days.
Adults and children ≥40 kg: One 500 mg/125 mg dose taken three times a day.
Children <40 kg: 20 mg/5 mg/kg/day to 60 mg/15 mg/kg/day given in three divided doses.
Children may be treated with Co-Amoxiclav tablets, suspensions or paediatric sachets.
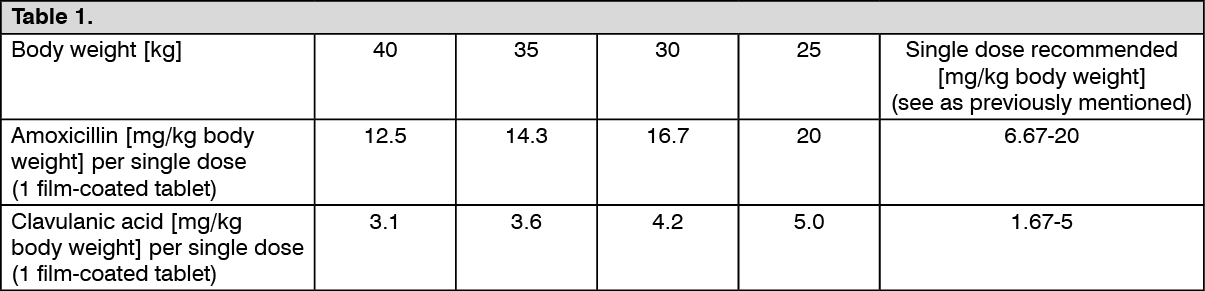
As the tablets cannot be divided, children weighing less than 25 kg must not be treated with Co-Amoxiclav tablets.
The table as follows presents the received dose (mg/kg body weight) in children weighing 25 kg to 40 kg upon administering a single 500/125 mg tablet. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Children aged 6 years and below or weighing less than 25 kg should preferably be treated with Co-Amoxiclav suspension or paediatric sachets.
No clinical data are available on doses of Co-Amoxiclav 4:1 formulations higher than 40 mg/10 mg/kg per day in children under 2 years.
Elderly: No dose adjustment is considered necessary.
Renal impairment: Dose adjustments are based on the maximum recommended level of amoxicillin.
No adjustment in dose is required in patients with creatinine clearance (CrCl) greater than 30 ml/min.
Adults and children ≥40 kg: (See Table 2.)
Click on icon to see table/diagram/image
Children <40 kg: (See Table 3.)
Click on icon to see table/diagram/image
Hepatic impairment: Dose with caution and monitor hepatic function at regular intervals.
Or as prescribed by the physician.
Symptoms and signs of overdose: Gastrointestinal symptoms and disturbance of the fluid and electrolyte balances may be evident. Amoxicillin crystalluria, in some cases leading to renal failure, has been observed.
Convulsions may occur in patients with impaired renal function or in those receiving high doses.
Amoxicillin has been reported to precipitate in bladder catheters, predominantly after intravenous administration of large doses. A regular check of patency should be maintained.
Treatment of intoxication: Gastrointestinal symptoms may be treated symptomatically, with attention to the water/electrolyte balance.
Amoxicillin/clavulanic acid can be removed from the circulation by haemodialysis.
Hypersensitivity to the active substances, to any of the penicillins or to any of the excipients.
History of a severe immediate hypersensitivity reaction (e.g. anaphylaxis) to another beta-lactam agent (e.g. a cephalosporin, carbapenem or monobactam).
History of jaundice/hepatic impairment due to amoxicillin/clavulanic acid.
Before initiating therapy with amoxicillin/clavulanic acid, careful enquiry should be made concerning previous hypersensitivity reactions to penicillins, cephalosporins or other beta-lactam agents.
Serious and occasionally fatal hypersensitivity hypersensitivity reactions (including anaphylactoid and severe cutaneous adverse reactions) have been reported in patients on penicillin therapy. These reactions are more likely to occur in individuals with a history of penicillin hypersensitivity and in atopic individuals. If an allergic reaction occurs, amoxicillin/clavulanic acid therapy must be discontinued and appropriate alternative therapy instituted.
In the case that an infection is proven to be due to an amoxicillin-susceptible organisms(s) then consideration should be given to switching from amoxicillin/clavulanic acid to amoxicillin in accordance with official guidance.
This presentation of Comxicla is not suitable for use when there is a high risk that the presumptive pathogens have reduced susceptibility or resistance to beta-lactam agents that is not mediated by beta-lactamases susceptible to inhibition by clavulanic acid. This presentation should not be used to treat penicillin-resistant S. pneumoniae.
Convulsions may occur in patients with impaired renal function or in those receiving high doses.
Amoxicillin/clavulanic acid should be avoided if infectious mononucleosis is suspected since the occurrence of a morbilliform rash has been associated with this condition following the use of amoxicillin.
Concomitant use of allopurinol during treatment with amoxicillin can increase the likelihood of allergic skin reactions.
Prolonged use may occasionally result in overgrowth of non-susceptible organisms.
The occurrence at the treatment initiation of a feverish generalised erythema associated with pustula may be a symptom of acute generalised exanthemous pustulosis (AGEP). This reaction requires Comxicla discontinuation and contraindicates any subsequent administration of amoxicillin.
Amoxicillin/clavulanic acid should be used with caution in patients with evidence of hepatic impairment.
Hepatic events have been reported predominantly in males and elderly patients and may be associated with prolonged treatment. These events have been very rarely reported in children. In all populations, signs and symptoms usually occur during or shortly after treatment but in some cases may not become apparent until several weeks after treatment has ceased. These are usually reversible. Hepatic events may be severe and, in extremely rare circumstances deaths have been reported. These have almost always occurred in patients with serious underlying disease or taking concomitant medications known to have the potential for hepatic effects.
Antibiotic-associated colitis has been reported with nearly all antibacterial agents including amoxicillin and may range in severity from mild to life threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhoea during or subsequent to the administration of any antibiotics. Should antibiotic-associated colitis occur, amoxicillin/clavulanic acid should immediately be discontinued, a physician be consulted and an appropriate therapy initiated. Anti-peristaltic medicinal products are contraindicated in this situation.
Periodic assessment of organ system functions, including renal, hepatic and haematopoietic function is advisable during prolonged therapy.
Prolongation of prothrombin time has been reported rarely in patients receiving amoxicillin/clavulanic acid. Appropriate monitoring should be undertaken when anticoagulants are prescribed concomitantly. Adjustments in the dose of oral anticoagulants may be necessary to maintain the desired level of anticoagulation.
In patients with renal impairment, the dose should be adjusted according to the degree of impairment.
In patients with reduced urine output, crystalluria has been observed very rarely, predominantly with parenteral therapy. During the administration of high doses of amoxicillin, it is advisable to maintain adequate fluid intake and urinary output in order to reduce the possibility of amoxicillin crystalluria. In patients with bladder catheters, a regular check of patency should be maintained.
During treatment with amoxicillin, enzymatic glucose oxidase methods should be used whenever testing for the presence of glucose in urine because false positive results may occur with non-enzymatic methods.
The presence of clavulanic acid in Comxicla may cause a non-specific binding of IgG and albumin by red cell membranes leading to a false positive Coombs test.
There have been reports of positive test results using the Bio-Rad Laboratories Platelia Aspergillus EIA test in patients receiving amoxicillin/clavulanic acid who were subsequently found to be free of Aspergillus infection. Cross-reactions with non-Aspergillus polysaccharides and polyfuranoses with Bio-Rad Laboratories Platelia Aspergillus EIA test have been reported. Therefore, positive test results in patients receiving amoxicillin/clavulanic acid should be interpreted cautiously and confirmed by other diagnostic methods.
Pregnancy: Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development. Limited data on the use of amoxicillin/clavulanic acid during pregnancy in humans do not indicate an increased risk of congenital malformations. In a single study in women with preterm, premature rupture of the foetal membrane it was reported that prophylactic treatment with amoxicillin/clavulanic acid may be associated with an increased risk of necrotising enterocolitis in neonates. Use should be avoided during pregnancy, unless considered essential by the physician.
Lactation: Both substances are excreted into breast milk (nothing is known of the effects of clavulanic acid on the breast-fed infant). Consequently, diarrhoea and fungus infection of the mucous membranes are possible in the breast-fed infant, so that breast-feeding might have to be discontinued. The possibility of sensitisation should be taken into account. Amoxicillin/clavulanic acid should only be used during breast-feeding after benefit/risk assessment by the physician in charge.
The most commonly reported adverse drug reactions (ADRs) are diarrhoea, nausea and vomiting.
The ADRs derived from clinical studies and post-marketing surveillance with Augmentin, sorted by MedDRA System Organ Class are listed as follows.
The following terminologies have been used in order to classify the occurrence of undesirable effects: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data). (See Table 4.)
Click on icon to see table/diagram/image
Oral anticoagulants: Oral anticoagulants and penicillin antibiotics have been widely used in practice without reports of interaction. However, in the literature there are cases of increased international normalised ratio in patients maintained on acenocoumarol or warfarin and prescribed a course of amoxicillin. If co-administration is necessary, the prothrombin time or international normalised ratio should be carefully monitored with the addition or withdrawal of amoxicillin. Moreover, adjustments in the dose of oral anticoagulants may be necessary.
Methotrexate: Penicillins may reduce the excretion of methotrexate causing a potential increase in toxicity.
Probenecid: Concomitant use of probenecid is not recommended. Probenecid decreases the renal tubular secretion of amoxicillin.
Concomitant use of probenecid may result in increased and prolonged blood levels of amoxicillin but not of clavulanic acid.
Mycophenolate mofetil: In patients receiving mycophenolate mofetil, reduction in pre-dose concentration of the active metabolite mycophenolic acid (MPA) of approximately 50% has been reported following commencement of oral amoxicillin plus clavulanic acid. The change in pre-dose level may not accurately represent changes in overall MPA exposure. Therefore, a change in the dose of mycophenolate mofetil should not normally be necessary in the absence of clinical evidence of graft dysfunction. However, close clinical monitoring should be performed during the combination and shortly after antibiotic treatment.
Store at temperatures not exceeding 30°C.
J01CR02 - amoxicillin and beta-lactamase inhibitor ; Belongs to the class of penicillin combinations, including beta-lactamase inhibitors. Used in the systemic treatment of infections.
Comxicla FC tab 625 mg
20's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image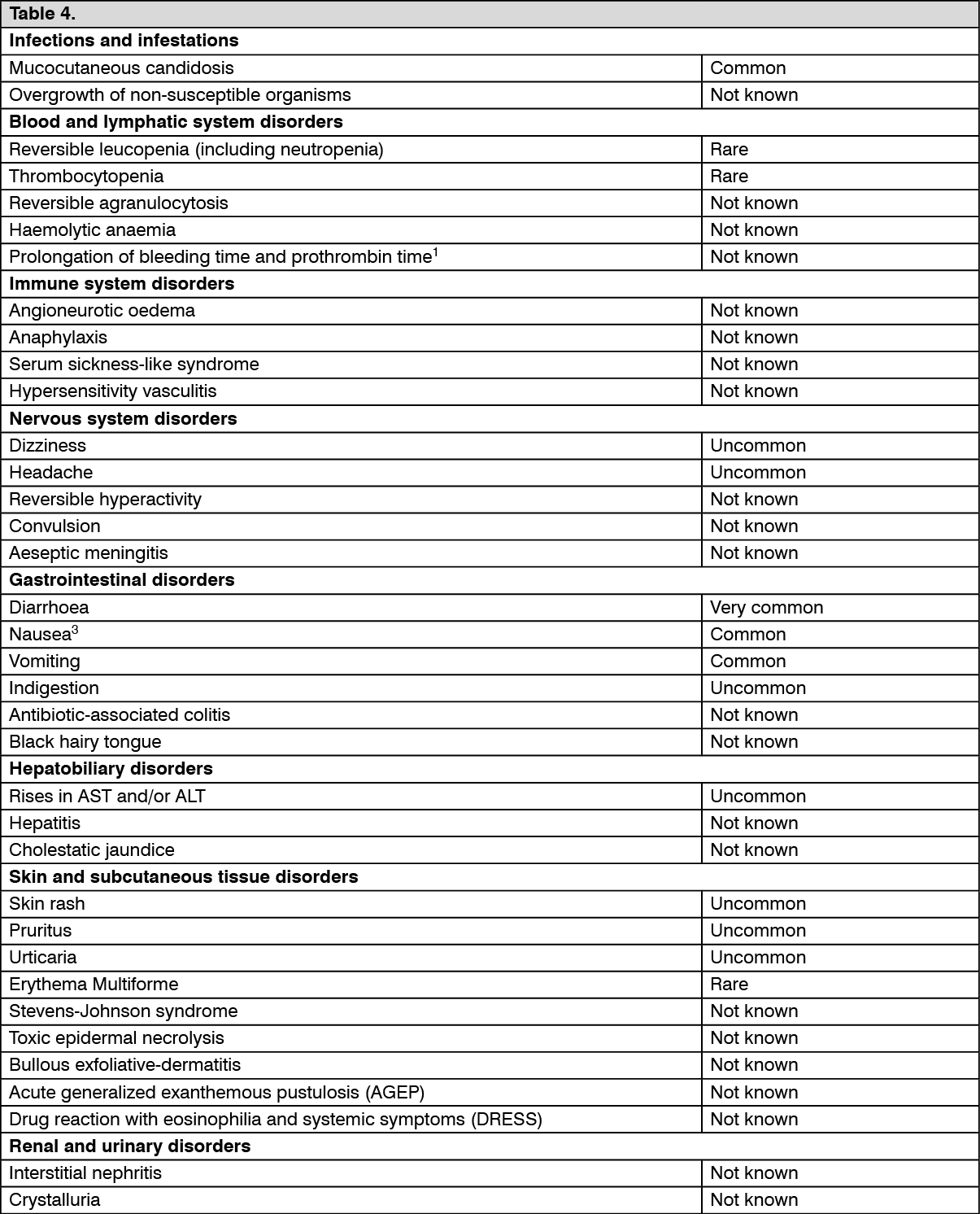 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out