Antibacterial.
Pharmacology: Pharmacodynamics: Cefepime hydrochloride (Cepiram) is a bactericidal agent that acts by inhibition of bacterial cell wall synthesis. Cefepime hydrochloride (Cepiram) has a broad spectrum of in vitro activity that encompasses a wide range of gram-positive and gram-negative bacteria. Cefepime hydrochloride (Cepiram) has a low affinity for chromosomally encoded beta-lactamases. It is highly resistant to hydrolysis by most beta-lactamases and exhibits rapid penetration into gram-negative bacterial cells. Within bacterial cells, the molecular targets of Cefepime are the penicillin binding proteins (PBP).
Cefepime hydrochloride (Cepiram) has shown to be active against most strains of the following microorganisms.
Aerobic Gram-Negative Microorganisms: Enterobacter; Escherichia coli; Klebsiella pneumoniae; Proteus mirabilis; Pseudomonas aeruginosa.
Aerobic Gram-Positive Microorganisms: Staphylococcus aureus (methicillin-susceptible isolates only)
; Streptococcus pneumoniae; Streptococcus pyogenes (Lancefield's Group A streptococci); Viridans group streptococci.
The following
in vitro data are available, but their clinical significance is unknown. Cefepime has been shown to have
in vitro activity against most isolates of the following microorganisms; however, the safety and effectiveness of cefepime in treating clinical infections due to these microorganisms have not been established in adequate and well-controlled trials.
Aerobic Gram-Positive Microorganisms: Staphylococcus epidermidis (methicillin-susceptible isolates only);
Staphylococcus saprophyticus; Streptococcus agalactiae (Lancefield's Group B streptococci).
Note: Most isolates of enterococci, eg,
Enterococcus faecalis, and methicillin-resistant staphylococci are resistant to cefepime.
Aerobic Gram-Negative Microorganisms: Acinetobacter calcoaceticus subsp. lwoffii;
Citrobacter diversus; Citrobacter freundii; Enterobacter agglomerans; Haemophilus influenzae (including beta-lactamase producing isolates);
Hafnia alvei; Klebsiella oxytoca; Moraxella catarrhalis (including beta-lactamase producing isolates);
Morganella morganii; Proteus vulgaris; Providencia rettgeri; Providencia stuartii; Serratia marcescens.
Note: Cefepime is inactive against many isolates of Stenotrophomonas (formerly
Xanthomonas maltophilia and
Pseudomonas maltophilia).
Anaerobic Microorganisms: Note: Cefepime is inactive against most isolates of
Clostridium difficile.
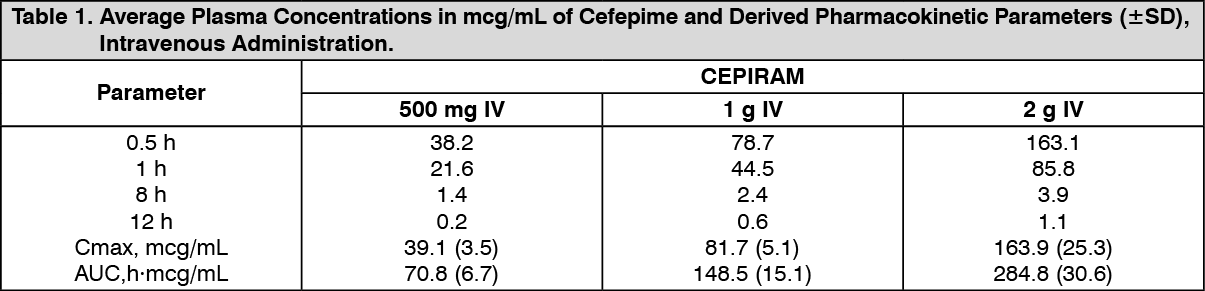
Pharmacokinetics: The average plasma concentrations of Cefepime hydrochloride (Cepiram) observed in healthy adult male volunteers at various times following single 30-minute infusions (IV) of Cefepime hydrochloride (Cepiram) 500 mg, 1 g and 2 g are summarized in Table 1. Elimination of Cepiram is principally via renal excretion with an average (+SD) half-life of 2.0 (+0.3) hours and total body clearance of 120.0 (+8.0) mL/min in healthy volunteers.
Cefepime hydrochloride (Cepiram) pharmacokinetics are linear over the range of 250 mg to 2 g.
There is no evidence of accumulation. The average steady state volume of distribution of Cefepime hydrochloride (Cepiram) is 18.0 (+2.0) L. The serum protein binding of Cefepime hydrochloride (Cepiram) is approximately 20% and is independent of its concentration in serum.
Cefepime hydrochloride (Cepiram) is excreted unchanged in the urine which accounts for approximately 85% of the administered dose. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Following administration of 250 mg IV peak concentration of 18 μg/mL are achieved. Following intramuscular (IM) administration, cefepime is completely absorbed. The average plasma concentrations of cefepime at various times following a single intramuscular injection are summarized in Table 2. The pharmacokinetics of cefepime are linear over the range of 500 mg to 2 g intramuscularly and do not vary with respect to treatment duration. (See Table 2.)
Click on icon to see table/diagram/image
Distribution: The average steady-state volume of distribution of cefepime is 18 (±2) L. The serum protein binding of cefepime is approximately 20% and is independent of its concentration in serum.
Metabolism and Excretion: Cefepime is metabolized to N-methylpyrrolidine (NMP) which is rapidly converted to the N-oxide (NMP-N-oxide). Urinary recovery of unchanged cefepime accounts for approximately 85% of the administered dose. Less than 1% of the administered dose is recovered from urine as NMP, 6.8% as NMP-N-oxide, and 2.5% as an epimer of cefepime. Because renal excretion is a significant pathway of elimination, patients with renal dysfunction and patients undergoing hemodialysis require dosage adjustment.
Specific Populations: Renal impairment: The average half-life in patients requiring hemodialysis was 13.5 (±2.7) hours and in patients requiring continuous peritoneal dialysis was 19 (±2) hours. Cefepime total body clearance decreased proportionally with creatinine clearance in patients with abnormal renal function, which serves as the basis for dosage adjustment recommendations in this group of patients.
Hepatic impairment: The pharmacokinetics of cefepime were unaltered in patients with hepatic impairment.
Geriatric patients: There appeared to be a decrease in cefepime total body clearance as a function of creatinine clearance. Therefore, dosage administration of cefepime in the elderly should be adjusted as appropriate if the patient's creatinine clearance is 60 mL/min or less.
Pediatric patients: No accumulation was seen when cefepime was given at 50 mg per kg every 12 hours (n=13), while Cmax, AUC, and t½ were increased about 15% at steady state after 50 mg per kg every 8 hours. The exposure to cefepime following a 50 mg per kg intravenous dose in a pediatric patient is comparable to that in an adult treated with a 2 g intravenous dose.
Microbiology: Susceptibility Tests: Dilution Techniques: Quantitative methods are used to determine antimicrobial minimum inhibitory concentrations (MICs). The MIC values should be interpreted according to the following criteria: see Table 3.
Click on icon to see table/diagram/image
Diffusion techniques: Reports from the laboratory providing results of the standard single-disk susceptibility test with a 30-mg Cefepime hydrochloride (Cepiram) disk should be interpreted according to the following criteria: see Table 4.
Click on icon to see table/diagram/image



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image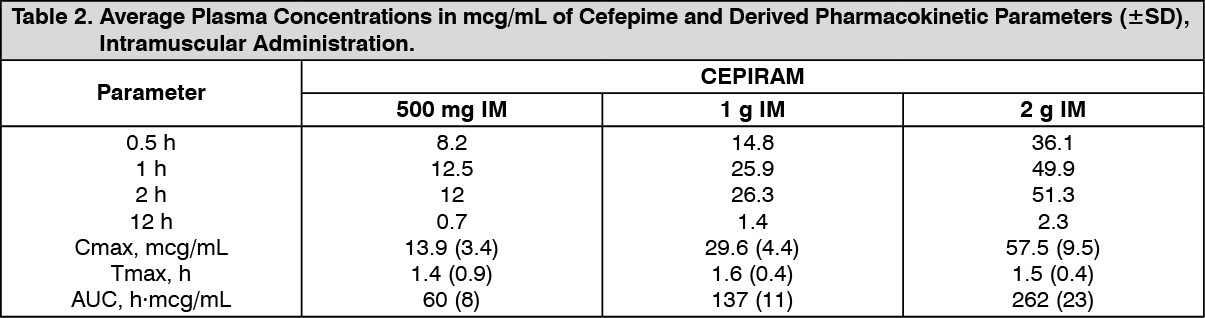 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image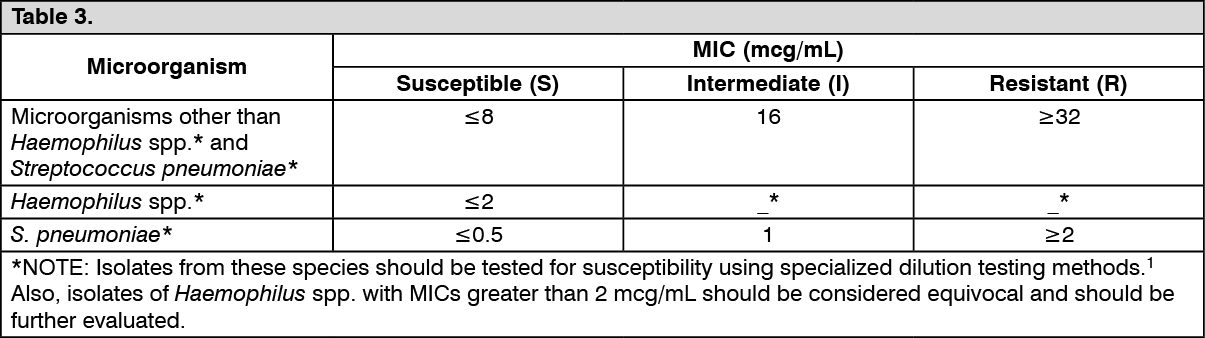 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image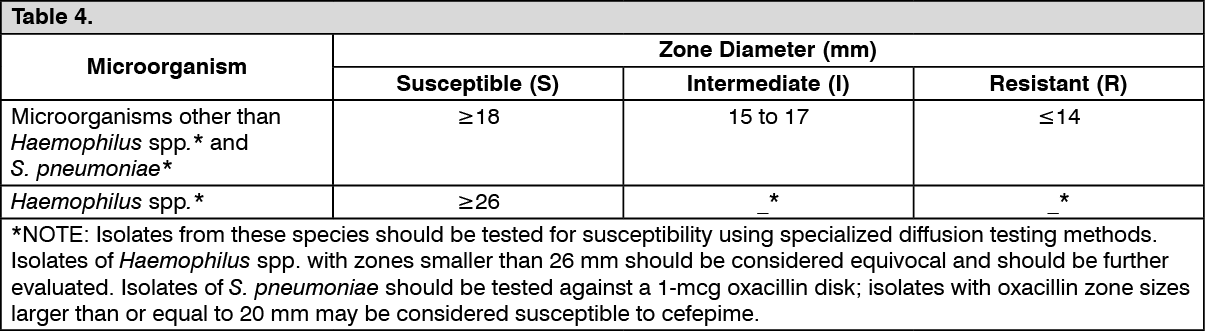 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image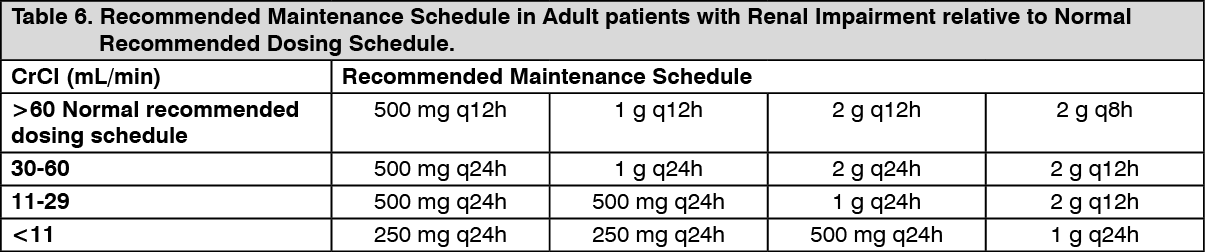 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out