Each film-coated tablet contains: Tadalafil 20 mg.
Excipients with known effect: Betacyclodextrin (E 459): This medicine contains 20 mg of cyclodextrin in each film-coated tablet.
Lactose: If the patient has been told by the doctor that the patient has an intolerance to some sugars, contact the doctor before taking this medicinal product. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Tartrazine (E 102): May cause allergic reactions.
Phosphodiesterase Type 5 (PDE-5) Inhibitor.
Pharmacology: Tadalafil is a selective, reversible inhibitor of cyclic guanosine monophosphate (cGMP)-specific phosphodiesterase type 5 (PDE5). When sexual stimulation causes the local release of nitric oxide, inhibition of PDE5 by tadalafil produces increased levels of cGMP in the corpus cavernosum. This results in smooth muscle relaxation and inflow of blood into the penile tissues, thereby producing an erection. Tadalafil has no effect in the absence of sexual stimulation.
Pharmacokinetics: Tadalafil is readily absorbed after oral administration and the mean maximum observed plasma concentration (Cmax) is achieved at a median time of 2 hours after dosing. Absolute bioavailability of tadalafil following oral dosing has not been determined. The rate and extent of absorption of tadalafil are not influenced by food, thus tadalafil may be taken with or without food. The time of dosing (morning versus evening) had no clinically relevant effects on the rate and extent of absorption. The mean volume of distribution is approximately 63 L, indicating that tadalafil is distributed into tissues. At therapeutic concentrations, 94% of tadalafil in plasma is bound to proteins. Protein binding is not affected by impaired renal function. Less than 0.0005% of the administered dose appeared in the semen of healthy subjects. Tadalafil is predominantly metabolized by the cytochrome P450 (CYP) 3A4 isoform. The major circulating metabolite is the methylcatechol glucuronide. This metabolite is at least 13,000-fold less potent than tadalafil for PDE5. Consequently, it is not expected to be clinically active at observed metabolite concentrations. The mean oral clearance for tadalafil is 2.5 L/h and the mean half-life is 17.5 hours in healthy subjects. Tadalafil is excreted predominantly as inactive metabolites, mainly in the feces (approximately 61% of the dose) and to a lesser extent in the urine (approximately 36% of the dose).
Treatment of erectile dysfunction in adult males.
In order for tadalafil to be effective, sexual stimulation is required.
Tadalafil is not indicated for use by women.
Adult men: In general, the recommended dose is 10 mg taken prior to anticipated sexual activity and with or without food. In those patients in whom tadalafil 10 mg does not produce an adequate effect, 20 mg might be tried. It may be taken at least 30 minutes prior to sexual activity. The maximum dose frequency is once per day.
Tadalafil 10 and 20 mg is intended for use prior to anticipated sexual activity and it is not recommended for continuous daily use.
Elderly men: Dose adjustments are not required in elderly patients.
Men with renal impairment: Dose adjustments are not required in patients with mild to moderate renal impairment. For patients with severe renal impairment, 10 mg is the maximum recommended dose. Once-daily dosing of tadalafil is not recommended in patients with severe renal impairment.
Men with hepatic impairment: The recommended dose of tadalafil is 10 mg taken prior to anticipated sexual activity and with or without food. There is limited clinical data on the safety of tadalafil in patients with severe hepatic impairment (Child-Pugh Class C); if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. There are no available data about the administration of doses higher than 10 mg of tadalafil to patients with hepatic impairment.
Men with diabetes: Dose adjustments are not required in diabetic patients.
Pediatric population: There is no relevant use of tadalafil in the pediatric population with regard to the treatment of erectile dysfunction.
Single doses of up to 500 mg have been given to healthy subjects, and multiple daily doses up to 100 mg have been given to patients. Adverse events were similar to those seen at lower doses. In cases of overdose, standard supportive measures should be adopted as required. Hemodialysis contributes negligibly to tadalafil elimination.
Hypersensitivity to the active substance or to any of the excipients.
In clinical studies, tadalafil was shown to augment the hypotensive effects of nitrates. This is thought to result from the combined effects of nitrates and tadalafil on the nitric oxide/cGMP pathway. Therefore, administration of tadalafil to patients who are using any form of organic nitrate is contraindicated.
Tadalafil must not be used in men with cardiac disease for whom sexual activity is inadvisable. Physicians should consider the potential cardiac risk of sexual activity in patients with pre-existing cardiovascular disease.
The coadministration of PDE5 inhibitors, including tadalafil, with guanylate cyclase stimulators, such as riociguat, is contraindicated as it may potentially lead to symptomatic hypotension.
Before treatment with tadalafil: A medical history and physical examination should be undertaken to diagnose erectile dysfunction and determine potential underlying causes, before pharmacological treatment is considered. Prior to initiating any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients, since there is a degree of cardiac risk associated with sexual activity. Tadalafil has vasodilator properties, resulting in mild and transient decreases in blood pressure and as such potentiates the hypotensive effect of nitrates. The evaluation of erectile dysfunction should include a determination of potential underlying causes and the identification of appropriate treatment following an appropriate medical assessment.
Cardiovascular: Serious cardiovascular events, including myocardial infarction, sudden cardiac death, unstable angina pectoris, ventricular arrhythmia, stroke, transient ischemic attacks, chest pain, palpitations and tachycardia, have been reported. In patients receiving concomitant antihypertensive medicinal products, tadalafil may induce a blood pressure decrease. When initiating daily treatment with tadalafil, appropriate clinical considerations should be given to a possible dose adjustment of the antihypertensive therapy. In patients who are taking alpha1 blockers, concomitant administration of tadalafil may lead to symptomatic hypotension in some patients. The combination of tadalafil and doxazosin is not recommended.
Vision: Visual defects and cases of non-arteritic anterior ischemic optic neuropathy (NAION) have been reported in connection with the intake of tadalafil and other PDE5 inhibitors. The patient should be advised that in case of sudden visual defect, the patient should stop taking tadalafil and consult a physician immediately.
Decreased or sudden hearing loss: Cases of sudden hearing loss have been reported after the use of tadalafil. Although other risk factors were present in some cases (such as age, diabetes, hypertension and previous hearing loss history) patients should be advised to stop taking tadalafil and seek prompt medical attention in the event of sudden decrease or loss of hearing.
Priapism and anatomical deformation of the penis: Patients who experience erections lasting 4 hours or more should be instructed to seek immediate medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency may result. Tadalafil, should be used with caution in patients with anatomical deformation of the penis (such as angulation, cavernosal fibrosis or Peyronie's disease), or in patients who have conditions which may predispose them to priapism (such as sickle cell anemia, multiple myeloma or leukemia).
Use with CYP3A4 inhibitors: Caution should be exercised when prescribing tadalafil to patients using potent CYP3A4 inhibitors (ritonavir, saquinavir, ketoconazole, itraconazole, and erythromycin) as increased tadalafil exposure (AUC) has been observed if the medicinal products are combined.
Tadalafil and other treatments for erectile dysfunction: The safety and efficacy of combinations of tadalafil and other PDE5 inhibitors or other treatments for erectile dysfunction have not been studied. The patients should be informed not to take tadalafil in such combinations.
Renal and hepatic impairment: Due to increased tadalafil exposure (AUC), limited clinical experience and the lack of ability to influence clearance by dialysis, once-a-day dosing of tadalafil is not recommended in patients with severe renal impairment.
Pregnancy Category B. Tadalafil is not indicated for use by women.
There are limited data from the use of tadalafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/fetal development, parturition or postnatal development. As a precautionary measure, it is preferable to avoid the use of tadalafil during pregnancy.
Available pharmacodynamic/toxicological data in animals have shown excretion of tadalafil in milk. A risk to the suckling child cannot be excluded. Tadalafil should not be used during breastfeeding.
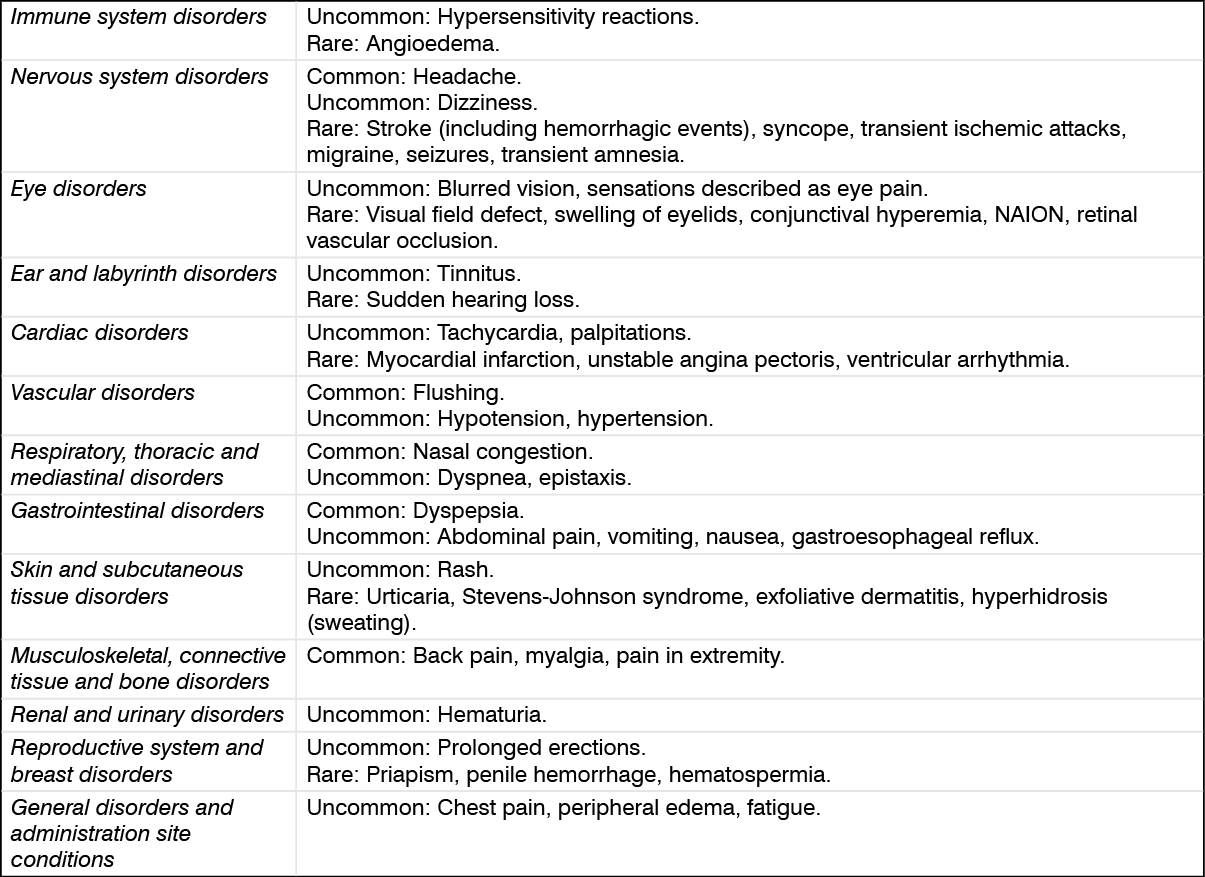
See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Seek medical attention immediately at the first sign of any adverse drug reaction.
Effects of other substances on tadalafil: Cytochrome P450 inhibitors: Tadalafil is principally metabolized by CYP3A4. A selective inhibitor of CYP3A4, ketoconazole, increased tadalafil exposure (AUC) and Cmax relative to the AUC and Cmax values for tadalafil alone. Ritonavir, a protease inhibitor, which is an inhibitor of CYP3A4, CYP2C9, CYP2C19, and CYP2D6, increased tadalafil AUC 2-fold with no change in Cmax. Although specific interactions have not been studied, other protease inhibitors, such as saquinavir, and other CYP3A4 inhibitors, such as erythromycin, clarithromycin, itraconazole and grapefruit juice should be co-administered with caution as they would be expected to increase plasma concentrations of tadalafil. Consequently, the incidence of the adverse reactions might be increased.
Transporters: The role of transporters (for example p-glycoprotein) in the disposition of tadalafil is not known. Therefore, there is the potential of drug interactions mediated by inhibition of transporters.
Cytochrome P450 inducers: A CYP3A4 inducer, rifampicin, reduced tadalafil AUC by 88%, relative to the AUC values for tadalafil alone. This reduced exposure can be anticipated to decrease the efficacy of tadalafil; the magnitude of decreased efficacy is unknown. Other inducers of CYP3A4 such as phenobarbital, phenytoin and carbamazepine, may also decrease plasma concentrations of tadalafil.
Effects of tadalafil on other drug products: Nitrates: In clinical studies, tadalafil (5, 10 and 20 mg) was shown to augment the hypotensive effects of nitrates. Therefore, administration of tadalafil to patients who are using any form of organic nitrate is contraindicated. In a patient prescribed any dose of tadalafil, where nitrate administration is deemed medically necessary in a life-threatening situation, at least 48 hours should have elapsed after the last dose of tadalafil before nitrate administration is considered. In such circumstances, nitrates should only be administered under close medical supervision with appropriate hemodynamic monitoring.
Antihypertensives (including calcium channel blockers): The coadministration of doxazosin and tadalafil increases the blood pressure-lowering effect of this alpha-blocker in a significant manner. This effect lasts at least twelve hours and may be symptomatic, including syncope. Therefore, this combination is not recommended. In interaction studies performed in a limited number of healthy volunteers, these effects were not reported with alfuzosin or tamsulosin. However, caution should be exercised when using tadalafil in patients treated with any alpha-blockers, and notably in the elderly. Treatments should be initiated at minimal dosage and progressively adjusted. In clinical pharmacology studies, the potential for tadalafil to augment the hypotensive effects of antihypertensive medicinal products was examined. Major classes of antihypertensive medicinal products were studied, including calcium channel blockers (amlodipine), angiotensin converting enzyme (ACE) inhibitors (enalapril), beta-adrenergic receptor blockers (metoprolol), thiazide diuretics (bendrofluazide), and angiotensin II receptor blockers (various types and doses, alone or in combination with thiazides, calcium channel blockers, beta-blockers, and/or alpha-blockers). Tadalafil had no clinically significant interaction with any of these classes. In patients receiving concomitant antihypertensive medicinal products, tadalafil 20 mg may induce a blood pressure decrease, which (with the exception of alpha blockers) is, in general, minor and not likely to be clinically relevant.
Riociguat: Concomitant use of riociguat with PDE5 inhibitors, including tadalafil, is contraindicated.
5-alpha reductase inhibitors: In a clinical trial that compared tadalafil 5 mg co-administered with finasteride 5 mg to placebo plus finasteride 5 mg in the relief of BPH symptoms, no new adverse reactions were identified. However, as a formal drug-drug interaction study evaluating the effects of tadalafil and 5-alpha reductase inhibitors (5-ARIs) has not been performed, caution should be exercised when tadalafil is co-administered with 5-ARIs.
CYP1A2 substrates (e.g. theophylline): When tadalafil 10 mg was administered with theophylline (a non-selective phosphodiesterase inhibitor) in a clinical pharmacology study, there was no pharmacokinetic interaction. The only pharmacodynamic effect was a small (3.5 bpm) increase in heart rate. Although this effect is minor and was of no clinical significance in this study, it should be considered when co-administering these medicinal products.
Ethinylestradiol and terbutaline: Tadalafil has been demonstrated to produce an increase in the oral bioavailability of ethinylestradiol; a similar increase may be expected with oral administration of terbutaline, although the clinical consequence of this is uncertain.
Alcohol: Alcohol concentrations were not affected by coadministration with tadalafil. In addition, no changes in tadalafil concentrations were seen 3 hours after coadministration with alcohol. Alcohol was administered in a manner to maximize the rate of alcohol absorption (overnight fast with no food until 2 hours after alcohol). Tadalafil did not augment the mean blood pressure decrease produced by alcohol but in some subjects, postural dizziness and orthostatic hypotension were observed. When tadalafil was administered with lower doses of alcohol, hypotension was not observed and dizziness occurred with similar frequency to alcohol alone. The effect of alcohol on cognitive function was not augmented by tadalafil.
Cytochrome P450 metabolized medicinal products: Tadalafil is not expected to cause clinically significant inhibition or induction of the clearance of medicinal products metabolized by CYP450 isoforms. Studies have confirmed that tadalafil does not inhibit or induce CYP450 isoforms, including CYP3A4, CYP1A2, CYP2D6, CYP2E1, CYP2C9 and CYP2C19. CYP2C9 substrates (e.g. R-warfarin) Tadalafil had no clinically significant effect on exposure (AUC) to S-warfarin or R- warfarin (CYP2C9 substrate), nor did tadalafil affect changes in prothrombin time induced by warfarin.
Aspirin: Tadalafil did not potentiate the increase in bleeding time caused by acetyl salicylic acid.
Store at temperatures not exceeding 30°C.
G04BE08 - tadalafil ; Belongs to the class of drugs used in erectile dysfunction.
Cedafil FC tab 20 mg
100's;10's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out