Dapagliflozin propanediol monohydrate, metformin hydrochloride.
Catania Plus: Yellow colored, oval shape, biconvex, film coated tablets, plain on both sides.
Each film-coated tablet contains: Dapagliflozin (as propanediol monohydrate 10 mg, Metformin HCl (in extended-release form) 500 mg.
Catania Max: Yellow colored, capsule shape, biconvex, film coated tablets, plain on both sides.
Each film-coated tablet contains: Dapagliflozin (as propanediol monohydrate) 10 mg, Metformin HCl (in extended-release form) 1 g.
Pharmacotherapeutic group: Drugs used in diabetes. Combinations of oral blood glucose-lowering drugs. ATC code: A10BD15.
Pharmacology: Mechanism of action: Dapagliflozin: Most of the reabsorption of filtered glucose from the tubular lumen is carried out by sodium-glucose cotransporter 2 (SGLT2), which is expressed in the proximal renal tubules. SGLT2 is inhibited by dapagliflozin. Dapagliflozin decreases the reabsorption of filtered glucose by blocking SGLT2, which encourages the excretion of glucose through the urine. Additionally, dapagliflozin enhances sodium transport to the distal tubule and decreases salt reabsorption. This may affect a number of physiological processes, such as reducing the heart's pre- and afterload, downregulating sympathetic activity, and lowering intraglomerular pressure, which is thought to be caused by an increase in tubuloglomerular feedback.
Metformin HCl: By reducing both basal and postprandial plasma glucose, the antihyperglycemic medication metformin helps people with type 2 diabetes mellitus improve their glucose tolerance. Metformin enhances insulin sensitivity by boosting peripheral glucose uptake and utilization while reducing intestinal glucose absorption and hepatic glucose synthesis. Insulin secretion is unaffected by metformin therapy, however fasting insulin levels and the daytime plasma insulin response may drop.
Pharmacodynamics: General: Dapagliflozin: After taking dapagliflozin, both healthy individuals and patients with type 2 diabetes mellitus showed increases in the amount of glucose expelled in their urine. Patients with type 2 diabetes mellitus who received dosages of 5 or 10 mg of dapagliflozin daily for 12 weeks excreted about 70 grams of glucose in their urine daily. The daily dosage of 20 mg of dapagliflozin was found to result in a near-maximum excretion of glucose. Urine volume increases as a result of dapagliflozin-induced glucose excretion in the urine. For the 10 mg dosage, the increase in urine glucose excretion typically returns to baseline after 3 days of stopping dapagliflozin.
Cardiac Electrophysiology: In a trial of healthy subjects, dapagliflozin did not cause a clinically significant lengthening of the QTc interval at daily doses up to 150 mg (15 times the recommended maximum dose). Furthermore, in healthy patients, single doses of dapagliflozin up to 500 mg (50 times the recommended maximum dose) did not result in any clinically significant change in QTc interval.
Pharmacokinetics: Both dapagliflozin and metformin extended-release were exposed to the same degree when Dapagliflozin and Metformin HCl (As Extended Release) Tablets was administered to healthy subjects following a typical meal as opposed to when they were fasting. The typical meal caused the peak plasma concentrations of dapagliflozin to decrease by 35% and to be delayed by 1 to 2 hours when compared to the fasted condition. It is not thought that this food impact has any clinical significance. When taking Dapagliflozin and Metformin HCl (As Extended Release) Tablets combo pills, food has no discernible impact on the pharmacokinetics of metformin.
Absorption: Dapagliflozin: When dapagliflozin is taken orally, the maximum plasma concentration (Cmax) is typically reached in two hours while fasting. As the dosage of dapagliflozin increases within the therapeutic dose range, the Cmax and AUC values rise proportionately. After a dose of 10 mg of dapagliflozin is administered, its absolute oral bioavailability is 78%. When dapagliflozin is administered with a high-fat meal, its Cmax can drop by as much as 50% and its Tmax can be prolonged by around an hour. However, the AUC remains unchanged when compared to the fasted condition. It is thought that these alterations are not clinically significant, and dapagliflozin can be taken with or without food.
Metformin HCl: Cmax is reached with a median value of 7 hours and a range of 4 to 8 hours after a single oral dose of metformin HCl extended-release. When the metformin HCl extended-release tablet was taken with food, the amount of metformin absorption (as shown by AUC) increased by almost 50%. Food had no effect on metformin's Cmax or Tmax. Peak plasma levels of metformin HCl extended-release tablets are about 20% lower than those of metformin HCl immediate-release tablets at the same dose, although the degree of absorption (as determined by AUC) is comparable between the two types of tablets.
Distribution: Dapagliflozin: About 91% of dapagliflozin is protein bound. Patients with hepatic or renal impairment do not have changed protein binding.
Metformin HCl: The apparent volume of distribution (V/F) of metformin after single oral dosages of immediate-release metformin 850 mg averaged 654 ± 358 L; however, distribution studies using extended-release metformin have not been carried out. Unlike sulfonylureas, which are more than 90% protein bound, metformin is only weakly linked to plasma proteins. Erythrocytes are where metformin divides.
Metabolism: Dapagliflozin: UGT1A9 is the primary mediator of dapagliflozin metabolism; CYP-mediated metabolism is a minor human clearance mechanism. The main result of dapagliflozin's extensive metabolism is the inactive metabolite dapagliflozin 3-O-glucuronide. Dapagliflozin 3-O-glucuronide is the main drug-related component in human plasma and made up 61% of a 50 mg [14C]-dapagliflozin dose.
Metformin HCl: Metformin does not undergo hepatic metabolism (no metabolites have been found in humans) or biliary excretion, according to intravenous single-dose trials conducted in healthy people.
No research has been done on the metabolism of extended-release metformin pills.
Elimination: Dapagliflozin: The renal route is principally responsible for the elimination of dapagliflozin and its associated metabolites. Urine and feces contain 75% and 21% of the total radioactivity after a single 50 mg dose of [14C]-dapagliflozin, respectively. Less than 2% of the dosage is eliminated as parent medication in the urine. About 15% of the dosage is eliminated as parent medication in the feces. After a single oral dose of dapagliflozin (10 mg), the mean plasma terminal half-life (t1/2) is roughly 12.9 hours.
Metformin HCl: The main method of metformin elimination is tubular secretion, as renal clearance is roughly 3.5 times higher than creatinine clearance. Within the first 24 hours after oral administration, the kidneys remove around 90% of the medication that has been absorbed, with a half-life of about 6.2 hours for plasma clearance. The elimination half-life in blood is roughly 17.6 hours, indicating that the erythrocyte bulk might constitute a distribution compartment.
Specific Populations: Geriatric Patients: Dapagliflozin: Age has no clinically significant impact on dapagliflozin systemic exposures, according to a population pharmacokinetic analysis.
Metformin HCl: Limited information from controlled pharmacokinetic trials of metformin in healthy older adults indicates that, in comparison to healthy young subjects, the total plasma clearance of metformin is reduced, the half-life is extended, and the Cmax is raised. These findings suggest that a change in renal function is the main cause of the aging-related shift in metformin pharmacokinetics.
Pediatric Patients: Dapagliflozin: Dapagliflozin's pharmacokinetics and pharmacodynamics (glucosuria) in children with type 2 diabetes mellitus between the ages of 10 and 17 were comparable to those seen in adults with the same level of renal function.
Metformin HCl: The geometric mean metformin Cmax and AUC difference between pediatric type 2 diabetes children (12-16 years of age) and gender- and weight-matched healthy adults (20-45 years of age), all with normal renal function, was less than 5% following the administration of a single oral metformin 500 mg tablet with food.
Male and Female Patients: Dapagliflozin: Gender had no clinically significant impact on systemic exposures to dapagliflozin, according to a population pharmacokinetic investigation.
Metformin HCl: When evaluated by gender, there were no significant differences in metformin pharmacokinetic parameters between patients with type 2 diabetes mellitus and healthy volunteers (males = 19, females = 16). Similarly, metformin's antihyperglycemic efficacy was similar in males and females in controlled clinical trials including patients with type 2 diabetes.
Racial or Ethnic Groups: Dapagliflozin: Race (White, Black or African American, or Asian) has no clinically significant impact on systemic exposures to dapagliflozin, according to a population pharmacokinetic analysis.
Metformin HCl: There have been no research on the pharmacokinetic characteristics of metformin by race. Whites (n=249), Black or African Americans (n=51), and Hispanic or Latino Ethnicity (n=24) all experienced similar antihyperglycemic effects from metformin in controlled clinical trials in patients with type 2 diabetes mellitus.
Patients with Renal Impairment: Dapagliflozin: Adult patients with type 2 diabetes mellitus who had mild, moderate, or severe renal impairment (as assessed by eGFR) at steady-state (20 mg once daily dapagliflozin for 7 days) had geometric mean systemic exposures of dapagliflozin that were, respectively, 45%, 100%, and 200% higher than those who had normal renal function. Patients with type 2 diabetes mellitus who had renal impairment and increased systemic exposure to dapagliflozin did not have a correspondingly higher 24-hour urine glucose excretion. Compared to patients with type 2 diabetes mellitus who had normal renal function, those with mild, moderate, and severe renal impairment had steady-state 24-hour urine glucose excretion that was 42%, 80%, and 90% lower, respectively. It is unknown how hemodialysis affects exposure to dapagliflozin.
Metformin HCl: Metformin's blood and plasma half-lives are longer and renal clearance is lower in patients with impaired renal function.
Patients with Hepatic Impairment: Dapagliflozin: Following a single dose of 10 mg dapagliflozin, the mean Cmax and AUC of dapagliflozin in adult patients with mild and moderate hepatic impairment (Child-Pugh classifications A and B) were up to 12% and 36% higher, respectively, than in healthy matched control subjects. Clinical significance was not attributed to these changes. Compared to healthy matched controls, the mean Cmax and AUC of dapagliflozin were up to 40% and 67% higher, respectively, in adult patients with severe hepatic impairment (Child-Pugh class C).
Metformin HCl: There are no known pharmacokinetic investigations of metformin in hepatic impairment patients.
Extended-release Dapagliflozin and Metformin hydrochloride (HCl) are recommended as a supplement to diet and exercise to help adults and children with type 2 diabetes mellitus who are 10 years of age or older achieve better glycemic control.
Dapagliflozin is indicated to reduce: The chance of heart failure hospitalization in persons with type 2 diabetes mellitus who also have several cardiovascular risk factors or existing cardiovascular disease (CVD).
People with heart failure (NYHA class II-IV) who have a lower ejection fraction are at risk for cardiovascular mortality and heart failure hospitalization.
The risk of end-stage kidney disease, cardiovascular death, hospitalization for heart failure, and a prolonged reduction in estimated glomerular filtration rate in people with chronic kidney disease at risk of progression.
Limitations of Use: It is not advised for people with type 1 diabetes mellitus to use Dapagliflozin and Metformin HCl (As Extended Release) Tablets to enhance their glycemic control.
Patients with type 2 diabetes mellitus are the only ones who can use Dapagliflozin and Metformin HCl (As Extended Release) Tablets for all indications due to the metformin HCl component.
Patients with polycystic kidney disease or those who need or have recently received immunosuppressive therapy for renal disease are not advised to use Dapagliflozin and Metformin HCl (As Extended Release) Tablets for the treatment of chronic kidney disease. It is not anticipated that Dapagliflozin and Metformin HCl (As Extended Release) Tablets would work well in these groups.
Recommended Administration: Once a day, take Dapagliflozin and Metformin HCl (As Extended Release) Tablets orally in the morning along with some food.
Never chew, cut, or crush Dapagliflozin and Metformin HCl (As Extended Release) Tablets; instead, swallow them whole.
Recommended Dosage: Determine the patient's starting Dapagliflozin and Metformin HCl (As Extended Release) Tablets dosage depending on their current treatment plan. Before beginning Dapagliflozin and Metformin HCl (As Extended Release) Tablets, patients receiving an evening dosage of metformin HCl extended-release should forgo their previous dose.
For patients 10 years of age and older who are not currently taking dapagliflozin, a starting dose of 5 mg once daily is advised in order to enhance glycemic control.
The recommended dosage of dapagliflozin for individuals with heart failure and chronic renal disease is 10 mg once a day.
The maximum recommended daily dosage of 10 mg dapagliflozin and 2,000 mg metformin HCl extended-release maybe exceeded, however dosage maybe changed based on effectiveness and tolerability.
Recommended Dosage in Patients with Renal Impairment: Patients with an estimated glomerular filtration rate (eGFR) of 45 mL/min/1.73 m2 or higher do not require a dosage adjustment for Dapagliflozin and Metformin HCl (As Extended Release) Tablets.
For patients with an eGFR between 30 and 45 mL/min/1.73 m2, starting Dapagliflozin and Metformin HCl (As Extended Release) Tablets is not advised. If eGFR consistently drops below this threshold, weigh the advantages and disadvantages of continuing treatment.
Patients with an eGFR of less than 45 mL/min/1.73 m2 are unlikely to benefit from dapagliflozin in terms of improved glycemic control.
It is not advised to start metformin HCl in patients whose eGFR is less than 45 mL/min/1.73 m2.
Patients with end-stage renal disease, dialysis, or an eGFR below 30 mL/min/1.73 m2 should not take dapagliflozin and metformin HCl (as extended release) tablets because of the metformin HCl component.
Discontinuation for Iodinated Contrast Imaging Procedures: Patients with a history of liver disease, alcoholism, or heart failure, as well as those who will receive intra-arterial iodinated contrast, should stop taking Dapagliflozin and Metformin HCl (As Extended Release) Tablets at the time of or before an iodinated contrast imaging procedure. 48 hours following the imaging procedure, reevaluate eGFR; if renal function is stable, resume taking Dapagliflozin and Metformin HCl (As Extended Release) tablets.
Temporary Interruption for Surgery: If at all possible, avoid taking Dapagliflozin and Metformin HCl (As Extended Release) Tablets for at least three days before undergoing major surgery or extended fasting procedures. Once the patient is clinically stable and has resumed oral intake, start taking Dapagliflozin and Metformin HCl (As Extended Release) tablets again.
Dapagliflozin: For more overdosage management advice in the event of an overdose, think about calling the National Poison Management and Control Center or a physician toxicologist. Hemodialysis's ability to remove dapagliflozin has not been investigated.
Metformin HCl: There have been cases of metformin HCl overdose, including consumption of more than 50 grams. In about 32% of metformin overdose instances, lactic acidosis has been documented. Under ideal hemodynamic circumstances, metformin can be dialyzed and cleared at a rate of up to 170 mL/min. Hemodialysis may therefore be helpful in clearing individuals with suspected metformin overdose of accumulated medication.
Dapagliflozin and Metformin HCl (As Extended Release) Tablets is contraindicated in patients with: end-stage renal disease, dialysis patients, or severe renal impairment (eGFR < 30 mL/min/1.73 m2).
History of a severe allergic reaction to any of the excipients in Dapagliflozin and Metformin HCl (As Extended Release) Tablets, dapagliflozin, or metformin HCl. Dapagliflozin has been linked to serious hypersensitivity responses, such as angioedema and anaphylaxis.
Diabetic ketoacidosis and other forms of acute or chronic metabolic acidosis, with or without coma. Insulin should be used to treat diabetic ketoacidosis.
Lactic Acidosis: There have been post-marketing cases of metformin-associated lactic acidosis, including fatal cases. These cases had a subtle onset and were accompanied by non-specific symptoms such as malaise, myalgias, abdominal pain, respiratory distress, or increased somnolence; however, hypothermia, hypotension and resistant bradyarrhythmias have occurred with severe acidosis.
Diabetic Ketoacidosis in Patients with Type 1 Diabetes Mellitus and Other Ketoacidosis: Consider ketone monitoring in patients at risk for ketoacidosis, as indicated. Assess for ketoacidosis regardless of presenting blood glucose levels and discontinue Dapagliflozin and Metformin HCl (As Extended Release) Tablets if ketoacidosis is suspected. Monitor patients for resolution of ketoacidosis before restarting.
Volume Depletion: Before initiating Dapagliflozin and Metformin HCl (As Extended Release) Tablets, assess and correct volume status in the elderly, patients with renal impairment or low systolic blood pressure, and in patients on diuretics. Monitor for signs and symptoms during therapy.
Urosepsis and Pyelonephritis: Evaluate patients for signs and symptoms of urinary tract infections and treat promptly, if indicated.
Hypoglycemia: Consider a lower dosage of insulin or an insulin secretagogue to reduce the risk of hypoglycemia when used concomitantly with Dapagliflozin and Metformin HCl (As Extended Release) Tablets.
Necrotizing Fasciitis of the Perineum (Fournier's Gangrene): Serious, life-threatening cases have occurred in both females and males. Assess patients presenting with pain or tenderness, erythema, or swelling in the genital or perineal area, along with fever or malaise. If suspected, institute prompt treatment.
Vitamin B12 Deficiency: Metformin may lower vitamin B12 levels. Measure hematological parameters annually.
Genital Mycotic Infections: Monitor and treat if indicated.
Renal Impairment: Individuals with an eGFR of less than 45 mL/min/1.73 m2 are not advised to initiate Dapagliflozin and Metformin HCl (As Extended Release) Tablets, and individuals receiving dialysis, end-stage renal disease, or severe renal impairment (eGFR <30 mL/min/1.73 m2) are contraindicated.
Dapagliflozin: In the DAPA-CKD trial, 4304 adult patients with chronic kidney disease (eGFR 25 to 75 mL/min/1.73 m2) were assessed for dapagliflozin 10 mg. In the DAPA-HF trial, 1926 adult patients with an eGFR of 30 to 60 mL/min/1.73 m2 were also assessed for dapagliflozin 10 mg. Across all eGFR subgroups, dapagliflozin's safety profile matched the established safety profile.
Adult patients with moderate renal impairment (eGFR of 45 to less than 60 mL/min/1.73 m2 and an eGFR of 30 to less than 60 mL/min/1.73 m2) were included in two glycemic control trials that assessed dapagliflozin 10 mg. When taking dapagliflozin 10 mg, patients with diabetes and renal impairment are more likely to have hypotension and may be more vulnerable to acute kidney injury due to volume depletion. Thirteen patients who received dapagliflozin suffered bone fractures in the trial of adult patients with an eGFR of 30 to less than 60 mL/min/1.73 m2, but none of the patients who received a placebo did. When eGFR is less than 45 mL/min/1.73 m2, dapagliflozin 10 mg should not be used for glycemic control in patients without known CV disease or CV risk factors.
Metformin HCl: Metformin is largely eliminated by the kidney, and the more severe the renal impairment, the higher the chance of metformin buildup and lactic acidosis. When a patient's estimated glomerular filtration rate (eGFR) is less than 30 mL/min/1.73 m2, Dapagliflozin and Metformin HCl (As Extended Release) Tablets is contraindicated.
Hepatic Impairment: Some incidences of lactic acidosis have been linked to the use of metformin in patients with hepatic impairment. It is not advised to use Dapagliflozin and Metformin HCl (As Extended Release) Tablets in people who have liver impairment.
Use in Children: Pediatric patients ten years of age and older have demonstrated the safety and efficacy of Dapagliflozin and Metformin HCl (As Extended Release) Tablets as a supplement to diet and exercise to enhance glycemic control in type 2 diabetes mellitus.
Pediatric pharmacokinetic studies, trials in adults with type 2 diabetes mellitus, and a 26-week placebo-controlled trial of dapagliflozin with a 26-week extension in 157 pediatric patients aged 10 to 17 years are all in favor of using Dapagliflozin and Metformin HCl (As Extended Release) Tablets for this indication. Dapagliflozin's safety profile in pediatric patients with type 2 diabetes mellitus was comparable to that of adults in the placebo-controlled trial.
In children under the age of ten, the safety and efficacy of Dapagliflozin and Metformin HCl (As Extended Release) Tablets for glycemic control in individuals with type 2 diabetes mellitus have not been proven.
It has not been demonstrated that Dapagliflozin and Metformin HCl (As Extended Release) Tablets is safe or effective in lowering the risk of; hospitalization for heart failure in those with several cardiovascular risk factors or existing cardiovascular disease (CVD) and type 2 diabetes mellitus.
Heart failure hospitalization and cardiovascular death in individuals with heart failure (NYHA class II-IV) who have a lower ejection fraction.
Patients with chronic renal disease at risk of progression may experience persistent declines in their estimated glomerular filtration rate, end-stage kidney disease, cardiovascular mortality, and heart failure hospitalization.
Use in the Elderly: Dapagliflozin and Metformin HCl (As Extended Release) Tablets: Age-based Dapagliflozin and Metformin HCl (As Extended Release) Tablets dosage changes are not advised. Elderly patients should have their renal function evaluated more frequently.
Dapagliflozin: In 21 double-blind, controlled clinical trials, 1424 (24%) of the 5936 patients treated with dapagliflozin were 65 years of age or older, and 207 (3.5%) were 75 years of age or older. These trials evaluated the effectiveness of dapagliflozin in enhancing glycemic control. Efficacy was comparable for patients under 65 and those 65 and older after adjusting for degree of renal function (eGFR). A greater percentage of individuals treated with dapagliflozin for glycemic control who were aged 65 and older experienced hypotension as an adverse response.
Safety and efficacy for patients 65 years of age and younger and those over 65 in the general population and patients with type 2 diabetes mellitus were comparable in the DAPA-HF and DAPA-CKD trials. Of the 4744 patients with heart failure with reduced ejection fraction (HFrEF) in the DAPA-HF trial, 2714 (57%) were over 65. 1211 (57%) of the 2139 individuals with HFrEF and type 2 diabetes mellitus were over 65. Of the 4304 patients with chronic renal disease in the DAPACKD trial, 1818 (42%) were over 65. 1399 (48%) of the 2906 patients with type 2 diabetes mellitus and chronic renal disease were over 65.
Metformin HCl: There were not enough elderly people in controlled clinical studies of metformin to ascertain whether their responses differed from those of younger patients. Due to the increased likelihood of lactic acidosis, concurrent disease or other medication therapy, and reduced hepatic, renal, or cardiac function, senior patients should generally have their dosages chosen carefully, starting at the low end of the dose range. In older individuals, evaluate renal function more often.
Pregnancy: Risk Summary: Dapagliflozin and Metformin HCl (As Extended Release) Tablets is not advised during the second and third trimesters of pregnancy due to animal research indicating negative kidney consequences.
There is not enough information available about Dapagliflozin and Metformin HCl (As Extended Release) Tablets or dapagliflozin in pregnant women to assess the risk of serious birth abnormalities or miscarriage. There is no conclusive evidence linking metformin use during pregnancy to a significant risk of miscarriage or birth defects. Poorly managed diabetes during pregnancy carries dangers for both the mother and the fetus.
In animal experiments, rats given dapagliflozin at all tested doses during a period of renal development equivalent to the late second and third trimesters of human pregnancy experienced adverse renal pelvic and tubule dilatations that were not entirely reversible; the lowest dose exposed rats to 15 times the clinical dose of 10 mg.
In women with pre-gestational diabetes whose HbA1c is more than 7%, the estimated baseline risk of significant birth abnormalities is 6-10%; in women whose HbA1c is higher than 10%, it has been reported to be as high as 20-25%. The suggested population's estimated background risk of miscarriage is unknown. The estimated background risk for significant birth abnormalities and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively, in the general population of the United States.
Clinical Considerations: Disease-associated maternal and/or embryofetal risk: The risk of diabetic ketoacidosis, preeclampsia, spontaneous abortions, preterm birth, and delivery difficulties is increased for mothers with poorly managed diabetes during pregnancy. Uncontrolled diabetes raises the chance of serious birth abnormalities, stillbirth, and morbidity associated with macrosomia in the fetus.
Lactation: Risk Summary: Dapagliflozin and Metformin HCl (As Extended Release) Tablets presence in human milk, their effects on breastfed infants, and their impact on milk production are all unknown.
According to a small number of published studies, human milk contains metformin. Nevertheless, nothing is known about how metformin affects breastfed infants, and there is no evidence on how it affects milk production. The milk of nursing rats contains dapagliflozin. The clinical significance of these findings is unclear, nevertheless, because lactation physiology varies by species. The growing human kidney may be at danger since human kidney maturation takes place in utero and throughout the first two years of life, when lactational exposure may occur.
Advise women that using Dapagliflozin and Metformin HCl (As Extended Release) Tablets while nursing is not advised due to the possibility of severe adverse effects in breastfed infants.
Females and Males of Reproductive Potential: Talk to premenopausal women about the possibility of an unwanted pregnancy because metformin medication may cause some anovulatory women to ovulate.
Throughout the labeling, the following significant adverse reactions are explained: Lactic Acidosis.
Diabetic Ketoacidosis in Patients with Type 1 Diabetes Mellitus and Other Ketoacidosis.
Volume Depletion.
Urosepsis and Pyelonephritis.
Hypoglycemia with Concomitant Use with Insulin and Insulin Secretagogues.
Necrotizing Fasciitis of the Perineum (Fournier's Gangrene).
Vitamin B
12 Concentrations.
Genital Mycotic Infections.
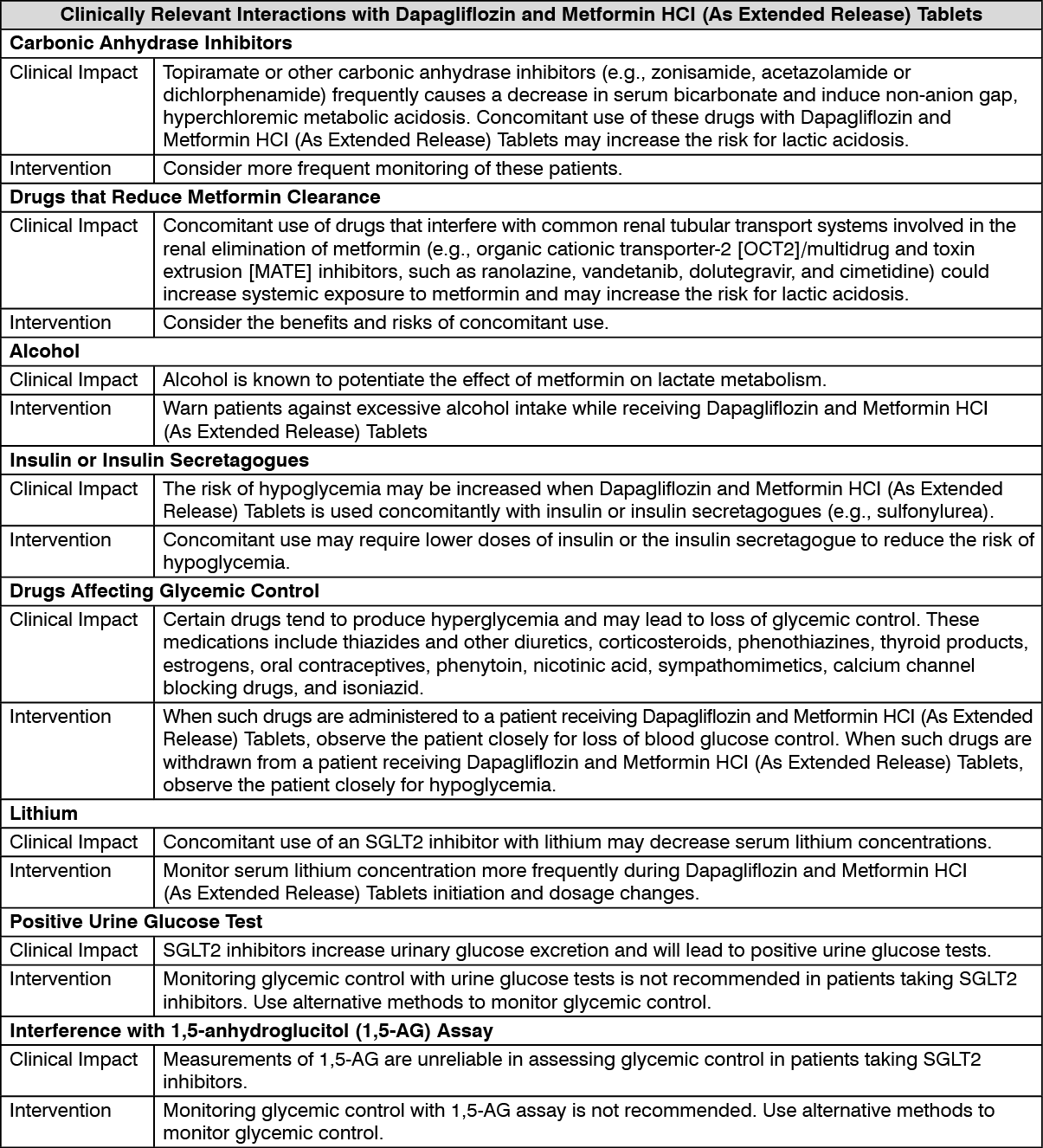
Interaction with other medicinal products and other forms of interaction: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Special Precautions for Handling and Disposal: No special requirements.
Store at a temperature not exceeding 30°C.
Shelf life: 36 months.
A10BD15 - metformin and dapagliflozin ; Belongs to the class of combinations of oral blood glucose lowering drugs. Used in the treatment of diabetes.
Catania Max 10 mg/1 g FC tab
30's
Catania Plus 10 mg/500 mg FC tab
30's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out