



 Sign Out
Sign Out
Ticagrelor has an additional mechanism of action, increasing local endogenous adenosine levels by inhibiting equilibrative nucleoside transporter-1 (ENT-1). Adenosine is formed locally at sites of hypoxia and tissue damage through degradation of released adenosine tri- and di-phosphate (ATP and ADP). As adenosine degradation is essentially restricted to the intracellular space, inhibition of ENT-1 by ticagrelor prolongs the half-life of adenosine and thereby increases its local extracellular concentration providing enhanced local adenosine responses. Ticagrelor has no clinically significant direct effect on adenosine receptors (A1, A2A, A2B, A3 and is not metabolised to adenosine. Adenosine has been documented to have a number of effects that include: vasodilation, cardioprotection, platelet inhibition, modulation of inflammation and induction of dyspnoea, which may contribute to the clinical profile of ticagrelor.
Onset of Action: In patients with stable coronary artery disease on ASA, Ticagrelor demonstrates a rapid onset of pharmacological effect as demonstrated by a mean Inhibition of Platelet Aggregation (IPA) for Ticagrelor at 0.5 hours after 180 mg loading dose of about 41%, with the maximum IPA effect of 87.9% to 89.6% by 2-4 hours post dose. 90% of patients had final extent IPA >70% by 2 hours post dose. The high IPA effect of Ticagrelor between 87%-89% was maintained between 2-8 hours.
Offset of Effect: After the Ticagrelor and the active metabolite concentrations decline to a level less than that required for receptor saturation, IPA gradually decreases with declining plasma concentrations. Since Ticagrelor bind reversibly, the recovery of platelet function does not depend on replacement of platelets. Ticagrelor has a faster rate of offset of IPA as compared to clopidogrel as determined by the slope of offset from 4-72 hours after last dose.
Median final extent IPA measured after the last dose of Ticagrelor is approximately 20-30% higher for Ticagrelor compared to clopidogrel. However, by 24 hours post-dose, %IPA is similar between Ticagrelor and clopidogrel, and is lower for Ticagrelor from 72 hours through 7 days compared with the clopidogrel. Mean %IPA for Ticagrelor at 72 hour (Day 3) post last dose was comparable to Day 5, and %IPA for Ticagrelor at Day 5 was similar to clopidogrel at Day 7, which is not statistically different from placebo.
Responders to Ticagrelor: IPA induced by Ticagrelor has less variability at peak plasma concentrations of Ticagrelor and the active metabolite observed with the 90 mg b.i.d. dose compared to clopidogrel. Patients with stable coronary artery disease predetermined to have low IPA response to clopidogrel, and given a concomitant dose of ASA, exhibited higher mean IPA response after administration of Ticagrelor as compared to clopidogrel. In non-responders to clopidogrel, the IPA response to Ticagrelor was observed to be higher and more consistent. Ticagrelor treatment resulted in consistently higher IPA compared with clopidogrel, and this was apparent post dose for both responders and non-responders.
Switching Data: Switching from clopidogrel to Ticagrelor results in an absolute IPA increase of 26.4% and switching from Ticagrelor to clopidogrel results in an absolute IPA decrease of 24.5%. Patients can be switched from clopidogrel to Ticagrelor without interruption of anti-platelet effect.
Adenosine mechanism (ENT-1): Ticagrelor increases plasma adenosine concentrations in ACS patients and has been shown to augment several physiological responses to adenosine. Adenosine is a vasodilator; ticagrelor has been shown to augment adenosine-induced coronary blood flow increases in healthy volunteers and ACS patients. Adenosine is an endogenous platelet inhibitor; ticagrelor has been shown to augment adenosine-mediated inhibition of platelet aggregation in addition to platelet inhibition due to its P2Y12 antagonism. Adenosine has been linked to the cardioprotective effect of preconditioning; ticagrelor has been shown to reduce infarct size via an adenosine-mediated mechanism in a rat model of reperfusion injury. Adenosine also includes dyspnoea in healthy volunteers. Thus, the dyspnoea observed in some patients taking ticagrelor may partly or completely be mediated by adenosine.
Clinical efficacy: The clinical evidence for the efficacy of Ticagrelor is derived from the PLATO [PLATelet Inhibition and Patient Outcomes] study, a comparison of Ticagrelor to clopidogrel, both given in combination with acetylsalicylic acid (ASA) and other standard therapy.
The PLATO study was an 18,624 patient randomized, double-blind, parallel group, phase III, efficacy and safety study of Ticagrelor compared with clopidogrel for prevention of vascular events in patients with Acute Coronary Syndromes (unstable angina, non ST elevation, Myocardial Infarction [NSTEMI] or ST elevation Myocardial Infarction [STEMI].
The study was comprised of patients who presented within 24 hours of onset of the most recent episode of chest pain or symptoms. Patients were randomized to receive clopidogrel (756 mg once daily, with an initial loading dose of 300 mg if previous thienopyridine therapy had not been given). An additional loading dose of 300 mg was allowed at investigator discretion, or a loading dose of 180 mg of Ticagrelor followed by a maintenance dose of 90 mg of Ticagrelor twice daily. Patients could have been medically managed, treated with percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG).
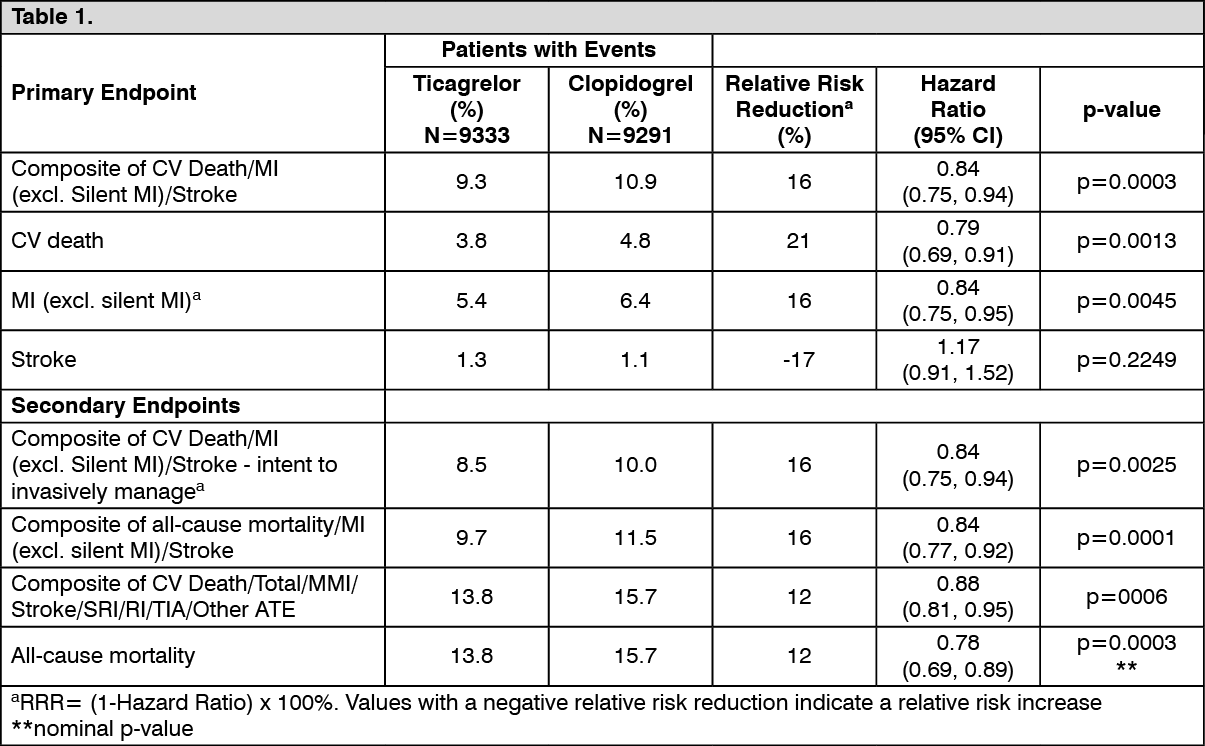
Daily, with an initial loading dose of 300 mg if previous thienopyridine therapy had not been given. An additional loading dose of 300 mg was allowed at investigator discretion, or a loading dose of 180 mg of Ticagrelor followed by a maintenance dose of 90 mg of Ticagrelor twice daily. Patients could have been medically managed, treated with percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTicagrelor is superior to clopidogrel in the prevention of thrombotic events (RRR 16%, ARR 1.9%, NNT =54) of the composite efficacy endpoint (cardiovascular (CV) death, myocardial infarction (MI) and stroke) over 12 months. The difference in treatments was driven by cardiovascular death and myocardial infarction with no difference on strokes. Ticagrelor demonstrated a statistically significant relative risk reduction of 16% (ARR 1.1%) for MI and a 21% relative risk reduction (ARR 1.1%) for CV death. Treating 91 patients with Ticagrelor instead of clopidogrel will prevent 1 CV death.
Ticagrelor showed superiority to clopidogrel in preventing the composite endpoint (cardiovascular [CV] death, myocardial infarction [MI], or stroke). This result appeared early (absolute risk reduction [ARR] 0.6% and Relative Risk Reduction [RRR] of 12% at 30 days), with a constant treatment effect over the entire 12 month period, yielding ARR 1.9% per year with RRR of 16%. This suggests it is appropriate to treat for at least 12 months.
In PLATO a large number of subgroup comparisons were conducted for the primary efficacy endpoint to assess the robustness and consistency of the overall benefit. The treatment effect of Ticagrelor over clopidogrel appears consistent across multiple patient subgroups by demographic characteristics including weight, gender, medical history, concomitant therapy, and by final index event diagnosis (STEMI, NSTEMI and UA).
A weakly significant treatment interaction was observed with region whereby the HR for the primary endpoint favours Ticagrelor in the rest of world but favours clopidogrel in North America, which represented approximately 10% of the overall population studied (interaction p-value=0.045).
This apparent treatment-by-region interaction observed in PLATO could plausibly be attributed to chance, at least in part. Additional analyses suggest that the efficacy of Ticagrelor relative to clopidogrel is associated with ASA dose during maintenance therapy. The data show greater efficacy of Ticagrelor compared to clopidogrel, it is recommended that Ticagrelor compared to clopidogrel when used in conjunction. With low maintenance dose ASA (75-150 mg). The relative efficacy of Ticagrelor versus clopidogrel when used with high doses of ASA (>300 mg) is less certain. Based on this observed relationship between maintenance ASA dose and relative efficacy of Ticagrelor compared to clopidogrel, it is recommended that Ticagrelor is used with a low maintenance dose of ASA 75-150 mg.
The benefits associated with Ticagrelor were also independent of the use of other acute and long-term cardiovascular therapies, including heparin, low molecular weight heparin (LMWH), Intravenous GPIIB/IIIa inhibitors, lipid-lowering drugs, beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists, and proton pump inhibitors.
Ticagrelor demonstrated a statistically significant RRR of 16% (ARR 2.1%) for the composite of all-cause mortality, MI and stroke compared to clopidogrel.
The final secondary endpoint (all-cause mortality), MI and stroke compared to clopidogrel.
The final secondary endpoint (all cause mortality) was evaluated. Ticagrelor demonstrated a RRR of 22% for all-cause mortality compared to clopidogrel at a nominal significance level of p=0.0003 and an ARR of 1.4%.
Holter Substudy: To study the occurrence of ventricular pauses and other arrhythmic episodes during PLATO, investigators performed Holter monitoring in a subset of nearly 3000 patients, of whom approximately 2000 had recordings both in the acute phase of their ACS and after one month. The primary variable of interest was the occurrence of ventricular pauses ≥3 seconds. More patients had ventricular pauses with Ticagrelor (6.0%) than with clopidogrel (3.5%) in the acute phase; and 2.2% and 1.6% respectively after 1 month. More patients had ventricular pauses with Ticagrelor than with clopidogrel, however there were no adverse clinical consequences associated with this imbalance (including pacemaker insertions) in this population of patients.
Ticagrelor is orally active. Unlike clopidogrel, it does not require CYP450 enzyme activity to inhibit platelet aggregation. Polymorphisms in the gene coding for P-glycoprotein transport (ABCB1) may impact efficacy of both clopidogrel and Ticagrelor. In PLATO, 10,825 patients provided genetic samples for genotype determination of CYP2C19 and ABCB1 loci. An analysis provided these associations of genotype groupings on efficacy and safety outcomes in PLATO.
The superiority of Ticagrelor over clopidogrel is not significantly affected by patient CYP2C19 genotype.
Ticagrelor reduced major CV events compared to clopidogrel independently of CYP2C19 genotype.
Event rates for Ticagrelor did not vary with CYP2C19 genotype.
In clopidogrel treated group, CYP2C19 Loss of Function (LOF) allele carriers had increased primary endpoint event rates compared with non-carriers.
Similar to the overall PLATO study, Total Major Bleeding did not differ between Ticagrelor and clopidogrel regardless of CYP2C19 genotype, although patients with one or more Gain of Function (GOF) alleles on clopidogrel had the highest rate of major bleeding.
Similar to the overall PLATO study, Non-CABG bleeding was increased with Ticagrelor compared to clopidogrel in patients with a CYP2C19 LOF allele.
Non-CABG bleeding was similar with Ticagrelor and clopidogrel in patients with no CYP2C19 LOF allele.
Combined Efficacy and Safety Composite: A combined efficacy and safety composite (CV death, MI, stroke or PLATO-defined 'Total Major' bleeding) supports the clinical benefit of Ticagrelor compared to clopidogrel (RRR 8%, ARR 1.4%, HR 0.92; p=0.0257) over 12 months after ACS events.
Pharmacokinetics: General: Ticagrelor demonstrates linear pharmacokinetics and exposure to Ticagrelor and the active metabolite (AR-C124910XX) are approximately dose proportional.
Absorption: Absorption of Ticagrelor is rapid with a median Tmax of approximately 1.5 hours. The formation of the major circulating metabolite from Ticagrelor is rapid with a median Tmax of approximately 2.5 hours. The Cmax and AUC of Ticagrelor and the active metabolite increased in an approximately proportional manner with dose over the dose range studied (30-1260 mg).
The mean absolute bioavailability of Ticagrelor was estimated to be 36%, (range 25.4% to 64.0%). Ingestion of a high-fat meal had no effect on Ticagrelor Cmax or the AUC of the active metabolite, but resulted in a 21% increase in Ticagrelor AUC and 22% decrease in the active metabolite Cmax. These small changes are considered of minimal clinical significance; therefore, Ticagrelor can be given with or without food.
Ticagrelor as crushed tablets mixed in water, given orally or administered through a nasogastric tube into the stomach, is bioequivalent to whole tablets (AUC and Cmax within 80-125% for ticagrelor and the active metabolite). Initial exposure (0.5 and 1 hour post-dose) from crushed ticagrelor tablets mixed in water was higher compared to whole tablets, with a generally identical concentration profile thereafter (2 to 48 hours).
Distribution: The steady state volume of distribution of Ticagrelor is 87.5 L. Ticagrelor and the active metabolite is extensively bound to human plasma protein (>99.0%).
Metabolism: CYP3A is the major enzyme responsible for Ticagrelor metabolism and the formation of the active metabolite and their interactions with other CYP3A substrates ranges from activation through to inhibition. Ticagrelor and the active metabolite are weak P-glycoprotein inhibitors.
The major metabolite of Ticagrelor is AR-C124910XX, which is also active as assessed by in vitro binding to the platelet P2Y12 ADP-receptor. The systemic exposure to the active metabolite is approximately 30-40%.
Excretion: The primary route of Ticagrelor elimination is via hepatic metabolism. When radio labeled Ticagrelor is administered, the mean recovery of radioactivity is approximately 84% (57.8% in faeces, 26.5% in urine). Recoveries of Ticagrelor and the active metabolite in urine were both less than 1% of the dose. The primary route of elimination for the active metabolite is mostly via biliary secretion. The mean t1/2 was approximately 6.9 hours (range 4.5-12.8 hours) for Ticagrelor and 8.6 hours (range 6.5-12.8 hours) for the active metabolite.
Special Populations: Elderly: Higher exposures to Ticagrelor (approximately 60% for both Cmax and AUC) and the active metabolite (approximately 50% for both Cmax and AUC) were observed in elderly (≥65 years) subjects compared to younger subjects. These differences are not considered clinically significant.
Paediatric patients: Ticagrelor has not been evaluated in a paediatric population.
Sex: Higher exposures to Ticagrelor (approximately 52% and 37% for Cmax and AUC) were observed in women compared to men. These differences are not considered clinically significant.
Renal Impairment: Exposure to Ticagrelor was approximately 20% lower and exposure to the active metabolite was approximately 17% higher in patients with severe renal impairment compared to subjects with normal renal function. The IPA effect of Ticagrelor was similar between the two groups, however there was more variability observed in individual response in patients with severe renal impairment. No dosing adjustment is needed in patients with renal impairment. No information is available concerning treatment of patients on renal dialysis.
Hepatic Impairment: Cmax and AUC for Ticagrelor were 12% and 23% higher in patients with mild hepatic impairment compared to matched healthy subjects, respectively, however the IPA effect of Ticagrelor was similar between the two groups. No dose adjustment is needed for patients with mild hepatic impairment. Ticagrelor has not been studied in patients with moderate or severe hepatic impairment.
Race: Patients of Asian descent have a 39% higher mean bioavailability compared to Caucasian patients. Patients self-identified as Black had an 18% lower bioavailability of Ticagrelor compared to Caucasian patients. In clinical pharmacology studies, the exposure (Cmax and AUC) to Ticagrelor in Japanese subjects was approximately 40% (20% after adjusting for body weight) higher compared to that in Caucasians.