One tablet contains 2.5 mg terbutaline sulfate.
Pharmaco-therapeutical group: selective β2-agonist, terbutaline. ATC code: R03C C03.
Pharmacology: Pharmacodynamics: Terbutaline is an adrenergic agonist which predominantly stimulates β2-receptors, thus producing relaxation of bronchial smooth muscle, inhibition of the release of endogenous spasmogens, inhibition of edema caused by endogenous mediators, increased mucociliary clearance and relaxation of the uterine muscle.
The bronchodilating effect of Terbutaline sulfate (Bricanyl) tablets has in clinical trials been shown to have a duration for up to 8 hours.
Pharmacokinetics: There is a considerable first-pass metabolism in the intestinal wall and in the liver. The bioavailability is about 10% and increases to about 15% if terbutaline is taken on an empty stomach. Maximum plasma concentration of terbutaline is reached within 3 hours. Terbutaline is metabolized mainly by conjugation with sulphuric acid and excreted as the sulfate conjugate. No active metabolites are formed.
Toxicology: Preclinical safety data: The major toxic effect of terbutaline, observed in toxicological studies, is focal myocardial necrosis. This type of cardiotoxicity is a well-known class-effect, and the effect of terbutaline is similar to or less pronounced than that of other beta-receptor agonists.
Bronchial asthma. Chronic bronchitis, emphysema and other lung diseases where bronchospasm is a complicating factor.
Terbutaline sulfate (Bricanyl) tablets should be used as maintenance therapy in asthma and other pulmonary diseases where bronchospasm is a complicating factor. When used as maintenance therapy, the patient should also receive optimal anti-inflammatory therapy, e.g., inhaled corticosteroids, leukotriene receptor antagonists.
Dosage should be individualized.
Adults: During the first 1-2 weeks 2.5 mg (1 tablet) 3 times in a 24 h period is recommended. The dose may then, if necessary, be increased to 5 mg (2 tablets) 3 times in 24 hours.
Children: 0.075 mg/kg body weight 3 times in 24 hours. Not more than 5 mg (2 tablets) 3 times in 24 hours.
Possible symptoms and signs: Headache, anxiety, tremor, nausea, tonic muscle cramps, palpitations, tachycardia and cardiac arrhythmias. A fall in blood pressure sometimes occurs.
Laboratory findings: Hyperglycemia and lactacidosis sometimes occur. β2-agonists may cause hypokalemia as a result of redistribution of potassium.
Treatment of overdosage: Usually no treatment is required. If it can be suspected that significant amounts of terbutaline sulfate have been swallowed, the following measures should be considered: Gastric lavage, activated charcoal. Determine acid-base balance, blood glucose and electrolytes. Monitor heart rate and rhythm and blood pressure. The preferred antidote for overdosage with Terbutaline sulfate (Bricanyl) is a cardioselective beta-receptor blocking agent, but beta-receptor blocking drugs should be used with caution in patients with a history of bronchospasm. If the β2-mediated reduction in peripheral vascular resistance significantly contributes to the fall in blood pressure, a volume expander should be given.
Hypersensitivity to any of the ingredients.
As for all β2-agonists caution should be observed in patients with thyrotoxicosis.
Cardiovascular effects may be seen with sympathomimetic drugs, including Terbutaline sulfate (Bricanyl). There is some evidence from post-marketing data and published literature of myocardial ischaemia associated with beta agonists.
Patients with underlying severe heart disease (e.g. ischaemic heart disease, arrhythmia or severe heart failure) who are receiving Terbutaline sulfate (Bricanyl) should be warned to seek medical advice if they experience chest pain or other symptoms of worsening heart disease.
Attention should be paid to assessment of symptoms such as dyspnoea and chest pain, as they may be of either respiratory or cardiac origin.
Due to the hyperglycemic effects of β2-agonists, additional blood glucose controls are recommended initially in diabetic patients.
Potentially serious hypokalemia may result from β2-agonist therapy. Particular caution is recommended in acute severe asthma as the associated risk may be augmented by hypoxia. The hypokalemic effect may be potentiated by concomitant treatments (see Interactions). It is recommended that serum potassium levels are monitored in such situations.
Patients with persistent asthma who require maintenance therapy with β2-agonists should also receive optimal anti-inflammatory therapy, e.g., inhaled corticosteroids, leukotriene receptor antagonists. These patients must be advised to continue taking their anti-inflammatory therapy after the introduction of Terbutaline sulfate (Bricanyl) even when symptoms decrease. Should symptoms persist, or if treatment with β2-agonists needs to be increased, this indicates a worsening of the underlying condition and warrants a reassessment of the therapy.
Effects on ability to drive and use machines: Terbutaline sulfate (Bricanyl) does not affect the ability to drive or use machines.
No teratogenic effects have been observed in patients or in animals. However, caution is recommended during the first trimester of pregnancy.
Maintenance treatment with oral beta2-agonists for asthma and other pulmonary diseases should be used with caution at the end of pregnancy because of the potential tocolytic effect.
Terbutaline passes over to breast milk but an influence on the child is unlikely with therapeutic doses.
Transient hypoglycemia has been reported in newborn preterm infants after maternal β2-agonist treatment.
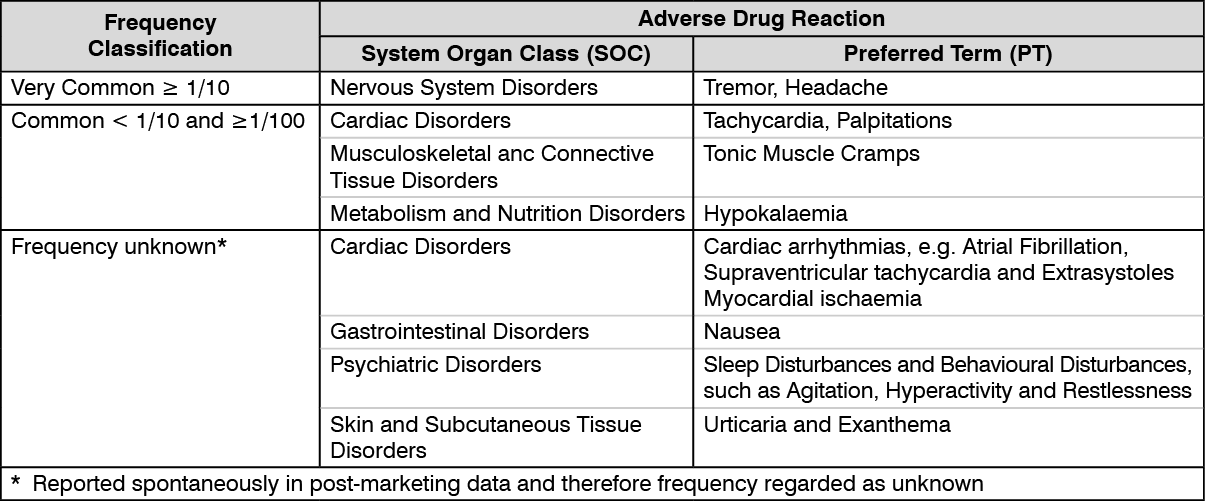
The intensity of the adverse reactions depends on dosage and route of administration. An initial dose titration will often reduce the adverse reactions. Most of the adverse reactions are characteristic of sympathomimetic amines. The majority of these effects have reversed spontaneously within the first 1-2 weeks of treatment. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Beta-receptor blocking agents (including eye-drops), especially those which are non-selective, may partly or totally inhibit the effect of beta-receptor stimulants.
Halogenated anaesthetics: Halothane anaesthesia should be avoided during β2-agonists treatment since it increases the risk of cardiac arrhythmias. Other halogenated anaesthetics should be used cautiously together with β2-agonists.
Potassium depleting agents and hypokalaemia: Owing to the hypokalaemic effect of beta-agonists, concurrent administration with Terbutaline sulfate (Bricanyl) of serum potassium depleting agents known to exacerbate the risk of hypokalaemia, such as diuretics, methyl xanthines and corticosteroids, should be administered cautiously after careful evaluation of the benefits and risks with special regard to the increased risk of cardiac arrhythmias arising as a result of hypokalaemia (see Precautions). Hypokalaemia also predisposes to digoxin toxicity.
Incompatibility: Not applicable.
Store at a temperature not exceeding 30°C.
R03CC03 - terbutaline ; Belongs to the class of adrenergics for systemic use, selective beta-2-adrenoreceptor agonists. Used in the treatment of obstructive airway diseases.
Bricanyl tab 2.5 mg
500's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out