Pharmacology: Pharmacodynamics: The pharmacodynamic action of ibandronic acid is inhibition of bone resorption. In vivo, ibandronic acid prevents experimentally induced bone destruction caused by cessation of gonadal function, retinoids, tumors or tumor extracts.
In young (fast growing) rats, the endogenous bone resorption is also inhibited, leading to increased bone mass compared with untreated animals. Animal models confirm that ibandronic acid is a highly potent inhibitor of osteoclastic activity. In growing rats, there was no evidence of impaired mineralization even at doses greater than 5,000 times the dose required for osteoporosis treatment.
The high potency and therapeutic margin of ibandronic acid allows for more flexible dosing regimens and intermittent treatment with long drug-free intervals at comparatively low doses.
Both daily and intermittent (with prolonged dose-free intervals) long-term administration in rats, dogs and monkeys were associated with formation of new bone of normal quality and/or increased mechanical strength even in doses in excess of any pharmacologically intended dose, including the toxic range.
In humans, the efficacy of both daily and intermittent administration with a dose-free interval of 9-10 weeks of ibandronic acid was confirmed in a clinical trial (MF 4411), in which Ibandronic acid demonstrated anti-fracture efficacy.
Both daily and intermittent (with a drug-free interval of 9-10 weeks per quarter) oral doses of Ibandronic acid in postmenopausal women produced biochemical changes indicative of dose-dependent inhibition of bone resorption, including suppression of urinary biochemical markers of bone collagen degradation (such as deoxypyridinoline, and cross-linked C- and N-telopeptides of type I collagen).
Following treatment discontinuation, there is a reversion to the pathological pre-treatment rates of elevated bone resorption associated with postmenopausal osteoporosis.
The histological analysis of bone biopsies after two and three years of treatment of postmenopausal women showed bone of normal quality and no indication of a mineralization defect.
In a Phase 1 bioequivalence study conducted in 72 postmenopausal women receiving 150 mg orally every 28 days for a total of four doses, inhibition in serum CTX following the first dose was seen as early as 24 hours post-dose (median inhibition 28%), with median maximal inhibition (69%) seen 6 days later. Following the third and fourth dose, the median maximum inhibition 6 days post dose was 74% with reduction to a median inhibition of 56% seen 28 days following the fourth dose. With no further dosing, there is a loss of suppression of biochemical markers of bone resorption.
Mechanism of Action: Ibandronic acid is a highly potent bisphosphonate belonging to the nitrogen-containing group of bisphosphonates, which act on bone tissue and specifically inhibit osteoclast activity. It does not interfere with osteoclast recruitment. The selective action of ibandronic acid on bone tissue is based on the high affinity of this compound for hydroxyapatite, which represents the mineral matrix of the bone.
Ibandronic acid reduces bone resorption, with no direct effect on bone formation. In postmenopausal women, it reduces the elevated rate of bone turnover towards premenopausal levels, leading to a progressive net gain in bone mass.
Daily or intermittent administration of ibandronic acid results in reduced bone resorption as reflected in reduced levels of serum and urinary biochemical markers of bone turnover, increased BMD and a decreased incidence of fractures.
Clinical/Efficacy Studies: Treatment of postmenopausal osteoporosis: In the initial three-year, randomized, double-blind, placebo-controlled, fracture study (MF 4411), a statistically significant and medically relevant decrease in the incidence of new radiographic morphometric and clinical vertebral fractures was demonstrated. Ibandronic acid was evaluated at oral doses of 2.5 mg daily and 20 mg intermittently (20 mg every other day for 12 doses at the start of each 3-month cycle, followed by a 9-10 week drug-free interval).
Ibandronic acid was taken 60 minutes before the first food or drink of the day (post-dose fasting period). The study enrolled 2,946 women aged 55 to 80 years (2,928 were eligible for efficacy), who were at least 5 years postmenopausal, who had a lumbar spine BMD 2 to 5 SD below the premenopausal mean (T-score) in at least one vertebra [L1-L4], and who had one to four prevalent vertebral fractures. All patients received 500 mg calcium and 400 IU vitamin D daily.
Ibandronic acid showed a statistically significant and medically relevant reduction in the incidence of new vertebral fracture with both regimens tested. The 2.5 mg daily regimen reduced the occurrence of new radiographic vertebral fractures by 62% over the three year duration of the study. Clinical vertebral fractures were also reduced by 49%. The strong effect on vertebral fractures was furthermore reflected by a statistically significant reduction of height loss compared to placebo.
The anti-fracture effect was consistent over the duration of the study.
There was no indication of a waning of the effect over time.
Although the clinical fracture trial for ibandronic acid was not specifically designed to demonstrate fracture efficacy in non-vertebral fractures, a relative risk reduction of similar magnitude (69%) as demonstrated for vertebral fractures was observed for non-vertebral fractures in a subgroup of patients being at higher fracture risk (femoral neck BMD T-score <-3.0 SD).
The observation of non-vertebral fracture efficacy in high-risk subgroups is consistent with clinical trial findings for other bisphosphonates.
Three-year lumbar spine BMD increase compared to placebo was 5.3% for the daily regimen. Compared to baseline this increase was 6.5%.
Biochemical markers of bone turnover (such as urinary CTX and serum osteocalcin) showed the expected pattern of suppression to premenopausal levels and reached maximum suppression within a period of 3-6 months. A clinically meaningful reduction of 50% and 78% of biochemical markers of bone resorption was observed as early as one month after start of treatment with Ibandronic acid 2.5 mg daily and 20 mg intermittently, respectively.
Decreases in biochemical markers of bone resorption were evident within 7 days of starting treatment.
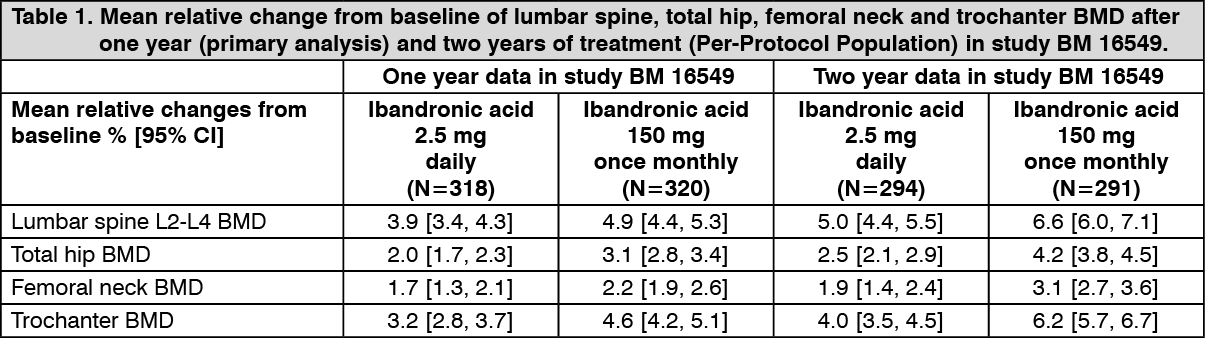
Ibandronic acid 150 mg once monthly: Bone mineral density: Ibandronic acid 150 mg once monthly was shown to be at least as effective as Ibandronic acid 2.5 mg daily at increasing BMD in a two year, double-blind, multicentre study (BM 16549) of postmenopausal women with osteoporosis (lumbar spine BMD T score below -2.5 SD at baseline). This was demonstrated in both the primary analysis at one year and in the confirmatory analysis at two years endpoint (Table 1). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Furthermore, Ibandronic acid 150 mg once monthly was proven superior to Ibandronic acid 2.5 mg daily for increases in lumbar spine BMD in a prospectively planned analysis at one year, p=0.002, and at two years, p<0.001.
At one year (primary analysis), 91.3% (p=0.005) of patients receiving Ibandronic acid 150 mg once monthly had a lumbar spine BMD increase above or equal to baseline (BMD responders), compared with 84.0% of patients receiving Ibandronic acid 2.5 mg daily. At two years, 93.5% (p=0.004) and 86.4% of patients receiving Ibandronic acid 150 mg once monthly or Ibandronic acid 2.5 mg daily, respectively, were responders.
For total hip BMD, 90.0% (p<0.001) of patients receiving Ibandronic acid 150 mg once monthly and 76.7% of patients receiving Ibandronic acid 2.5 mg daily had total hip BMD increases above or equal to baseline at one year. At two years 93.4% (p<0.001) of patients receiving Ibandronic acid 150 mg once monthly and 78.4%, of patients receiving Ibandronic acid 2.5 mg daily had total hip BMD increases above or equal to baseline.
When a more stringent criterion is considered, which combines both lumbar spine and total hip BMD, 83.9% (p<0.001) and 65.7% of patients receiving Ibandronic acid 150 mg once monthly or Ibandronic acid 2.5 mg daily, respectively, were responders at one year. At two years, 87.1% (p<0.001) and 70.5%, of patients met this criterion in the 150 mg monthly and 2.5 mg daily arms respectively.
Biochemical markers of bone turn-over Clinically meaningful reductions in serum CTX levels were observed at all time points measured, i.e. months 3, 6, 12 and 24. After one year (primary analysis) the median relative change from baseline was -76% for Ibandronic acid 150 mg once monthly and -67% for Ibandronic acid 2.5 mg daily.
At two years the median relative change was -68% and -62%, in the 150 mg monthly and 2.5 mg daily arms respectively.
At one year, 83.5% (p= 0.006) of patients receiving Ibandronic acid 150 mg once monthly and 73.9% of patients receiving Ibandronic acid 2.5 mg daily were identified as responders (defined as a decrease ≥50% from baseline).
At two years 78.7% (p=0.002) and 65.6% of patients were identified as responders in the 150 mg monthly and 2.5 mg daily arms respectively.
Based on the results of study BM 16549, Ibandronic acid 150 mg once monthly is expected to be at least as effective in preventing fractures as Ibandronic acid 2.5 mg daily.
Pharmacokinetics: The pharmacological effects of ibandronic acid are not directly related to actual plasma concentrations. This was demonstrated by various studies in animals and in humans, in which equivalent efficacy of ibandronic acid was demonstrated following either daily or intermittent regimens, consisting of a drug-free interval of several weeks (at least 6 weeks in rats, at least 11 weeks in dogs, at least 30 days in monkeys, and at least 9.5 weeks in humans) provided the same total dose was administered over this period.
Absorption: The absorption of ibandronic acid in the upper gastrointestinal tract is rapid after oral administration and plasma concentrations increase in a dose-proportional manner up to 50 mg oral intake, with greater than dose-proportional increases seen above this dose. Maximum observed plasma concentrations were reached within 0.5 to 2 hours (median 1 hour) in the fasted state and absolute bioavailability was about 0.6%. The extent of absorption is impaired when taken together with food or beverages (other than plain water). Bioavailability is reduced by about 90% when ibandronic acid is administered with a standard breakfast in comparison with bioavailability seen in fasted subjects. There is no meaningful reduction in bioavailability provided ibandronic acid is taken 60 minutes before a meal. Both bioavailability and BMD gains are reduced when food or beverage are taken less than 60 minutes after Ibandronic acid.
Distribution: After initial systemic exposure, ibandronic acid rapidly binds to bone or is excreted into urine. In humans, the apparent terminal volume of distribution is at least 90 l and the amount of dose reaching the bone is estimated to be 40-50% of the circulating dose.
Protein binding in human plasma is low (approximately 85% bound at therapeutic concentrations), and thus there is a low potential for drug-drug interaction due to displacement.
Metabolism: There is no evidence that ibandronic acid is metabolized in animals or humans.
Elimination: The absorbed fraction of ibandronic acid is removed from the circulation via bone absorption (40-50%) and the remainder is eliminated unchanged by the kidney.
The unabsorbed fraction of ibandronic acid is eliminated unchanged in the feces.
The range of observed apparent half-lives is broad and dependent on dose and assay sensitivity, but the apparent terminal half-life is generally in the range of 10-72 hours.
Early plasma levels fall quickly reaching 10% of peak values within 3 and 8 hours after intravenous or oral administration respectively.
Total clearance of ibandronic acid is low with average values in the range 84-160 ml/min.
Renal clearance (about 60 ml/min in healthy postmenopausal females) accounts for 50-60% of total clearance and is related to creatinine clearance.
The difference between the apparent total and renal clearances is considered to reflect the uptake by bone.
Pharmacokinetics in Special Populations: Gender: Bioavailability and pharmacokinetics of ibandronic acid are similar in both men and women.
Race: There is no evidence for clinically relevant interethnic differences between Asians and Caucasians in ibandronic acid disposition. There are few data available on patients of African origin.
Patients with renal impairment: Renal clearance of ibandronic acid in patients with various degrees of renal impairment is linearly related to creatinine clearance (CLcr). No dosage adjustment is necessary for patients with mild or moderate renal impairment (CLcr >30 ml/min), as shown in study BM 16549 where the majority of patients fell into these categories.
Subjects with severe renal impairment (CLcr ≤30 ml/min) receiving oral administration of 10 mg ibandronic acid daily for 21 days, had 2-3 fold higher plasma concentrations than subjects with normal renal function (total clearance = 129 ml/min). Total clearance of ibandronic acid was reduced to 44 ml/min in the subjects with severe renal impairment.
After i.v. administration of 0.5 mg, total, renal, and non-renal clearances decreased by 67%, 77% and 50%, respectively, in subjects with severe renal impairment.
However, there was no reduction in tolerability associated with the increase in exposure.
Patients with hepatic impairment: There are no pharmacokinetic data for ibandronic acid in patients who have hepatic impairment. The liver has no significant role in the clearance of ibandronic acid which is not metabolized but is cleared by renal excretion and by uptake into bone. Therefore, dosage adjustment is not necessary in patients with hepatic impairment. Further, as protein binding of ibandronic acid is low (85%) at therapeutic concentrations, hypoproteinemia in severe liver disease is unlikely to lead to clinically significant increases in free plasma concentration.
Elderly: In a multivariate analysis age was not found to be an independent factor of any of the pharmacokinetic parameters studied. As renal function decreases with age, this is the only factor to take into consideration (see Patients with renal impairment as previously mentioned).
Children: There are no data on the use of Ibandronic acid in patients less than 18 years old.
Toxicology: Preclinical Safety: Toxic effects in animals were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out