Summary Of The Safety Profile: The most commonly reported adverse reactions in placebo-controlled trials are akathisia and nausea each occurring in more than 3% of patients treated with oral aripiprazole.
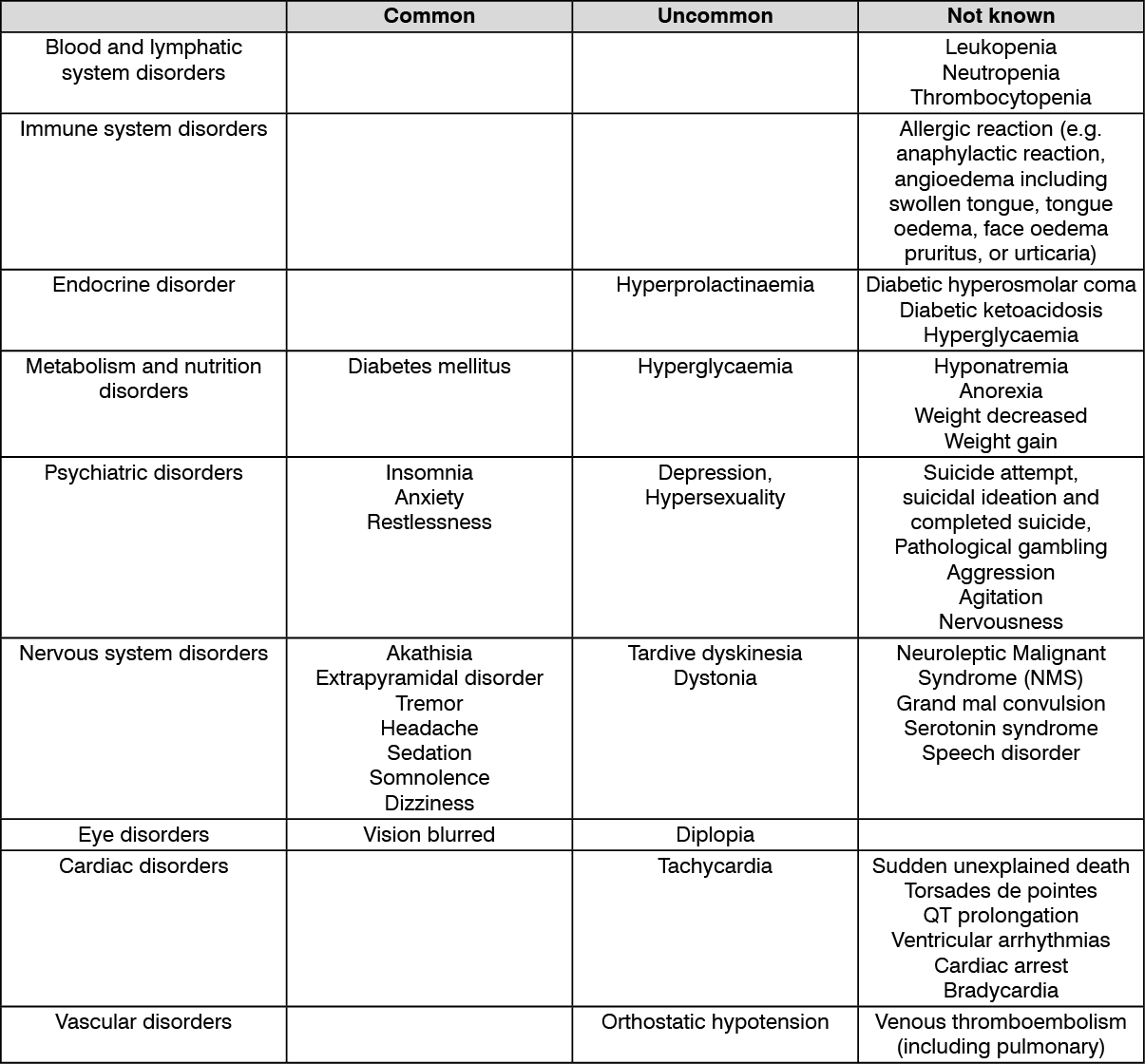
Tabulated List Of Adverse Reactions: All ADRs are listed by system organ class and frequency: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000) and not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness.
The frequency of adverse reactions reported during post-marketing use cannot be determined as they are derived from spontaneous reports. Consequently, the frequency of these adverse events is qualified as "not known". (See table.)
 Click on icon to see table/diagram/image
Description Of Selected Adverse Reactions: Extrapyramidal Symptoms (EPS):
Click on icon to see table/diagram/image
Description Of Selected Adverse Reactions: Extrapyramidal Symptoms (EPS): Schizophrenia: In a long term 52-week controlled trial, aripiprazole-treated patients had an overall-lower incidence (25.8%) of EPS including parkinsonism, akathisia, dystonia and dyskinesia compared with those treated with haloperidol (57.3%). In a long term 26-week placebo-controlled trial, the incidence of EPS was 19% for aripiprazole-treated patients and 13.1% for placebo-treated patients. In another long-term 26-week controlled trial, the incidence of EPS was 14.8% for aripiprazole-treated patients and 15.1% for olanzapine-treated patients.
Manic episodes in Bipolar I Disorder: In a 12-week controlled trial, the incidence of EPS was 23.5% for aripiprazole-treated patients and 53.3% for haloperidol-treated patients. In another 12-week trial, the incidence of EPS was 26.6% for patients treated with aripiprazole and 17.6% for those treated with lithium. In the long term 26-week maintenance phase of a placebo-controlled trial, the incidence of EPS was 18.2% for aripiprazole-treated patients and 15.7% for placebo-treated patients.
Akathisia: In placebo-controlled trials, the incidence of akathisia in bipolar patients was 12.1% with aripiprazole and 3.2% with placebo. ln schizophrenia patients the incidence of akathisia was 6.2% with aripiprazole and 3.0% with placebo.
Dystonia: Class Effect: Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible individuals during the first few days of treatment. Dystonic symptoms include: spasm of the neck muscles, sometimes progressing to tightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. While these symptoms can occur at low doses, they occur more frequently and with greater severity with high potency and at higher doses of first generation antipsychotic medicinal products. An elevated risk of acute dystonia is observed in males and younger age groups.
Prolactin: In clinical trials for the approved indications and post-marketing, both increase and decrease in serum prolactin as compared to baseline was observed with aripiprazole.
Laboratory Parameters: Comparisons between aripiprazole and placebo in the proportions of patients experiencing potentially clinically significant changes in routine laboratory and lipid parameters revealed no medically important differences. Elevations of CPK (Creatine Phosphokinase), generally transient and asymptomatic, were observed in 3.5% of aripiprazole treated patients as compared to 2.0% of patients who received placebo.
Paediatric Population: Schizophrenia in adolescents aged 15 years and older: In a short-term placebo-controlled clinical trial involving 302 adolescents (13-17 years) with schizophrenia, the frequency and type of undesirable effects were similar to those in adults except for the following reactions that were reported more frequently in adolescents receiving aripiprazole than in adults receiving aripiprazole (and more frequently than placebo): Somnolence/sedation and extrapyramidal disorder were reported very commonly (≥ 1/10), and dry mouth, increased appetite, and orthostatic hypotension were reported commonly (≥ 1/100, <1 /10). The safety profile in a 26-week open-label extension trial was similar to that observed in the short-term, placebo-controlled trial.
The safety profile of a long-term, double-blind placebo-controlled trial was also similar except for the following reactions that were reported more frequently than paediatric patients taking placebo: weight decreased, blood insulin increased, arrhythmia, and leukopenia were reported commonly (≥ 1/100, < 1/10).
In the pooled adolescent schizophrenia population (13-17 years) with exposure up to 2 years, incidence of low serum prolactin levels in females (<3 ng/ml) and males (< 2 ng/ml) was 29.5% and 48.3%, respectively. In the adolescent (13-17 years) schizophrenia population with aripiprazole exposure of 5 to 30 mg up to 72 months, incidence of low serum prolactin levels in females (<3 ng/ml) and males (< 2 ng/ml) was 25.6% and 45.0%, respectively.
In two long term trials with adolescent (13-17 years) schizophrenia and bipolar patients treated with aripiprazole, incidence of low serum prolactin levels in females (<3 ng/ml) and males (<2 ng/ml) was 37.0% and 59.4%, respectively.
Manic episodes in Bipolar I Disorder in adolescents aged 13 years and older: The frequency and type of undesirable effects in adolescents with Bipolar I Disorder were similar to those in adults except for the following reactions: very commonly (≥ 1/10) somnolence (23.0%), extrapyramidal disorder (18.4%), akathisia (16.0%), and fatigue (11.8%); and commonly (≥ 1/100, <1/10) abdominal pain upper, heart rate increased, weight increased, increased appetite, muscle twitching, and dyskinesia.
The following undesirable effects had a possible dose response relationship; extrapyramidal disorder (incidences were 10 mg, 9.1%, 30 mg, 28.8%, placebo, 1.7%); and akathisia (incidences were 10 mg, 12.1%, 30 mg, 20.3%, placebo, 1. 7%).
Mean changes in body weight in adolescents with Bipolar I Disorder at 12 and 30 weeks for aripiprazole were 2.4 kg and 5.8 kg, and for placebo 0.2 kg and 2.3 kg, respectively.
In the paediatric population somnolence and fatigue were observed more frequently in patients with bipolar disorder compared to patients with schizophrenia.
In the paediatric bipolar population (10-17 years) with exposure up to 30 weeks, incidence of low serum prolactin levels in females (< 3 ng/ml) and males (< 2 ng/ml) was 28.0% and 53.3%, respectively.
Reporting Of Suspected Adverse Reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product Healthcare professionals are asked to report any suspected adverse reactions.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out