Pink, modified rectangle, biconvex, film coated tablet with engraved 10 on one side and plain on the other.
Pharmacology: It has been proposed that Aripiprazole's efficacy in schizophrenia and Bipolar I Disorder is mediated through a combination of partial agonism at dopamine D2 and serotonin 5HT1a receptors and antagonism of serotonin 5HT2a receptors. Aripiprazole exhibited antagonist properties in animal models of dopaminergic hyperactivity and agonist properties in animal models of dopaminergic hypoactivity. Aripiprazole exhibited high binding affinity in vitro for dopamine D2 and D3, serotonin 5HT1a and 5HT2a receptors and moderate affinity for dopamine D4, serotonin 5HT2c and 5HT7, alpha-1 adrenergic and histamine H1 receptors. Aripiprazole also exhibited moderate binding affinity for the serotonin reuptake site and no appreciable affinity for muscarinic receptors. Interaction with receptors other than dopamine and serotonin subtypes may explain some of the other clinical effects of Aripiprazole.
Pharmacokinetics: Absorption: Aripiprazole is well absorbed, with peak plasma concentrations occurring within 3-5 hours after dosing. Aripiprazole undergoes minimal pre-systemic metabolism. The absolute oral bioavailability of the tablet formulation is 87%.
There is no effect of a high fat meal on the pharmacokinetics of Aripiprazole.
Distribution: Aripiprazole is widely distributed throughout the body with an apparent volume of distribution of 4.9 L/Kg, indicating extensive extravascular distribution. At therapeutic concentrations, Aripiprazole and dehydro-Aripiprazole are greater than 99% bound to serum proteins, binding primarily to albumin.
Biotransformation: Aripiprazole is extensively metabolized by the liver primarily by three biotransformation pathways: dehydrogenation, hydroxylation, and N-dealkylation. Based on in vitro studies, CYP3A4 and CYP2D6 enzymes are responsible for dehydrogenation and hydroxylation of Aripiprazole, and N-dealkylation is catalyzed by CYP3A4. Aripiprazole is the predominant medicinal product moiety in systemic circulation. At steady state, dehydro-Aripiprazole, the active metabolite, represents about 40% of Aripiprazole AUC in plasma.
Elimination: The mean elimination half-lives for Aripiprazole are approximately 75 hours in extensive metabolizers of CYP2D6 and approximately 146 hours in poor metabolizers of CYP2D6. The total body clearance of Aripiprazole is 0.7 mL/min/Kg, which is primarily hepatic. Following a single oral dose of [14C]-labelled Aripiprazole, approximately 27% of the administered radioactivity was recovered in the urine and approximately 60% in the feces. Less than 1% of unchanged Aripiprazole was excreted in the urine and approximately 18% was recovered unchanged in the feces.
Indicated for the treatment of schizophrenia in adults and in adolescents aged 15 years and older.
Indicated for the treatment of moderate to severe manic episodes in Bipolar I Disorder and for the prevention of a new manic episode in adults who experienced predominantly manic episodes and whose manic episodes responded to Aripiprazole treatment.
Indicated for the treatment up to 12 weeks of moderate to severe manic episodes in Bipolar I Disorder in adolescents aged 13 years and older.
Oral: Adults: Schizophrenia: The recommended starting dose for Aripiprazole is 10 or 15 mg/day with a maintenance dose of 15 mg/day administered on a once-a-day schedule without regard to meals.
Aripiprazole is effective in a dose range of 10 to 30 mg/day. Enhanced efficacy at doses higher than a daily dose of 15 mg has not been demonstrated although individual patients may benefit from a higher dose. The maximum daily dose should not exceed 30 mg.
Manic episodes in Bipolar I Disorder: The recommended starting dose for Aripiprazole is 15 mg administered on a once-a-day schedule without regard to meals as monotherapy or combination therapy. Some patients may benefit from a higher dose. The maximum daily dose should not exceed 30 mg.
Recurrence prevention of manic episodes in Bipolar I Disorder: For preventing recurrence of manic episodes in patients who have been receiving Aripiprazole as monotherapy or combination therapy, continue therapy at the same dose. Adjustments of daily dosage, including dose reduction should be considered on the basis of clinical status.
Pediatric population: Schizophrenia in adolescents aged 15 years and older: The recommended dose for Aripiprazole is 10 mg/day administered on a once-a-day schedule without regard to meals. Treatment should be initiated at 2 mg (using Aripiprazole oral solution 1 mg/mL) for 2 days, titrated to 5 mg for 2 additional days to reach the recommended daily dose of 10 mg. When appropriate, subsequent dose increases should be administered in 5 mg increments without exceeding the maximum daily dose of 30 mg.
Aripiprazole is effective in a dose range of 10 to 30 mg/day. Enhanced efficacy at doses higher than a daily dose of 10 mg has not been demonstrated although individual patients may benefit from a higher dose.
Aripiprazole is not recommended for use in patients with schizophrenia below 15 years of age due to insufficient data on safety and efficacy.
Manic episodes in Bipolar I Disorder in adolescents aged 13 years and older: The recommended dose for Aripiprazole is 10 mg/day administered on a once-a-day schedule without regard to meals. Treatment should be initiated at 2 mg (using Aripiprazole oral solution 1 mg/mL) for 2 days, titrated to 5 mg for 2 additional days to reach the recommended daily dose of 10 mg.
The treatment duration should be the minimum necessary for symptom control and must not exceed 12 weeks. Enhanced efficacy at doses higher than a daily dose of 10 mg has not been demonstrated, and a daily dose of 30 mg is associated with a substantially higher incidence of significant undesirable effects including EPS related events, somnolence, fatigue and weight gain. Doses higher than 10 mg/day should therefore only be used in exceptional cases and with close clinical monitoring.
Younger patients are at increased risk of experiencing adverse events associated with Aripiprazole. Therefore, Aripiprazole is not recommended for use in patients below 13 years of age.
Irritability associated with autistic disorder: The safety and efficacy of Aripiprazole in children and adolescents aged below 18 years have not yet been established.
Tics associated with Tourette's disorder: The safety and efficacy of Aripiprazole in children and adolescents 6 to 18 years of age have not yet been established.
Special population: Hepatic impairment: No dosage adjustment is required for patients with mild to moderate hepatic impairment. In patients with severe hepatic impairment, the data available are insufficient to establish recommendations. In these patients dosing should be managed cautiously. However, the maximum daily dose of 30 mg should be used with caution in patients with severe hepatic impairment.
Renal impairment: No dosage adjustment is required in patients with renal impairment.
Elderly: The effectiveness of Aripiprazole in the treatment of schizophrenia and Bipolar I Disorder in patients aged 65 years and older has not been established. Owing to the greater sensitivity of this population, a lower starting dose should be considered when clinical factors warrant.
Gender: No dosage adjustment is required for female patients as compared to male patients.
Smoking status: According to the metabolic pathway of Aripiprazole no dosage adjustment is required for smokers.
Dose adjustments due to interactions: When concomitant administration of potent CYP3A4 or CYP2D6 inhibitors with Aripiprazole occurs, the Aripiprazole dose should be reduced. When the CYP3A4 or CYP2D6 inhibitor is withdrawn from the combination therapy, Aripiprazole dose should then be increased.
When concomitant administration of potent CYP3A4 inducers with Aripiprazole occurs, the Aripiprazole dose should be increased. When the CYP3A4 inducer is withdrawn from the combination therapy, the Aripiprazole dose should then be reduced to the recommended dose.
Signs and symptoms: The potentially medically important signs and symptoms observed included lethargy, increased blood pressure, somnolence, tachycardia, nausea, vomiting and diarrhea. In addition, reports of accidental overdose with Aripiprazole alone (up to 195 mg) in children have been received with no fatalities. The potentially medically serious signs and symptoms reported included somnolence, transient loss of consciousness and extrapyramidal symptoms.
Management of overdose: Management of overdose should concentrate on supportive therapy, maintaining an adequate airway, oxygenation and ventilation, and management of symptoms. The possibility of multiple medicinal product involvement should be considered. Therefore, cardiovascular monitoring should be started immediately and should include continuous electrocardiographic monitoring to detect possible arrhythmias. Following any confirmed or suspected overdose with Aripiprazole, close medical supervision and monitoring should continue until the patient recovers.
Activated charcoal (50 g), administered one hour after Aripiprazole, decreased Aripiprazole Cmax by about 41% and AUC by about 51%, suggesting that charcoal may be effective in the treatment of overdose.
Hemodialysis: Although there is no information on the effect of hemodialysis in treating an overdose with Aripiprazole, hemodialysis is unlikely to be useful in overdose management since Aripiprazole is highly bound to plasma proteins.
Hypersensitivity to the active substance or to any of the excipients.
During antipsychotic treatment, improvement in the patient's clinical condition may take several days to some weeks. Patients should be closely monitored throughout this period.
Suicidality: The occurrence of suicidal behavior is inherent in psychotic illnesses and mood disorders and in some cases has been reported early after initiation or switch of antipsychotic treatment, including treatment with Aripiprazole. Close supervision of high-risk patients should accompany antipsychotic treatment.
Cardiovascular disorders: Aripiprazole should be used with caution in patients with known cardiovascular disease (history of myocardial infarction or ischemic heart disease, heart failure, or conduction abnormalities), cerebrovascular disease, conditions which would predispose patients to hypotension (dehydration, hypovolemia, and treatment with antihypertensive medicinal products) or hypertension, including accelerated or malignant. Cases of venous thromboembolism (VTE) have been reported with antipsychotic medicinal products.
Since patients treated with antipsychotics often present with acquired risk factors for VTE, all possible risk factors of VTE should be identified before and during treatment with Aripiprazole and preventive measures taken.
QT prolongation: Aripiprazole should be used with caution in patients with a family history of QT prolongation.
Tardive dyskinesia: If signs and symptoms of tardive dyskinesia appear in a patient on Aripiprazole, dose reduction or discontinuation should be considered. These symptoms can temporally deteriorate or even arise after discontinuation of treatment.
Other extrapyramidal symptoms: If signs and symptoms of other EPS appear in a patient taking Aripiprazole, dose reduction and dose clinical monitoring should be considered.
Neuroleptic Malignant Syndrome (NMS): NMS is potentially fatal symptom complex associated with antipsychotics. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis and cardiac dysrhythmia). Additional signs may include elevated creatinine phosphokinase, myoglobinuria (rhabdomyolysis), and acute renal failure. However, elevated creatine phosphokinase and rhabdomyolysis, not necessarily in association with NMS, have also been reported. If a patient develops signs and symptoms indicative of NMS, or presents with unexplained high fever without additional clinical manifestations of NMS, all antipsychotics, including Aripiprazole, must be discontinued.
Seizure: Aripiprazole should be used with caution in patients who have a history of seizure disorder or have conditions associated with seizures.
Elderly patients with dementia-related psychosis: Aripiprazole is not indicated for the treatment of patients with dementia-related psychosis due to increased mortality and cerebrovascular adverse reactions (e.g. stroke, transient ischemic attack).
Hyperglycemia and diabetes mellitus: Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics, including Aripiprazole. Risk factors that may predispose patients to severe complications include obesity and family history of diabetes.
Patients treated with any antipsychotics, including Aripiprazole, should be observed for signs and symptoms of hyperglycemia (such as polydipsia, polyuria, polyphagia and weakness) and patients with diabetes mellitus or with risk factors for diabetes mellitus should be monitored regularly for worsening of glucose control.
Hypersensitivity: Hypersensitivity reactions, characterized by allergic symptoms, may occur with Aripiprazole.
Weight gain: Weight gain is commonly seen in schizophrenic and bipolar mania patients due to co-morbidities, use of antipsychotics known to cause weight gain, poorly managed life-style, and might lead to severe complications. When seen, it is usually in those with significant risk factors such as history of diabetes, thyroid disorder or pituitary adenoma. If weight gain is clinically significant, dose reductions should be considered.
Dysphagia: Esophageal dysmotility and aspiration have been associated with the use of antipsychotics, including Aripiprazole.
Aripiprazole should be used cautiously in patients at risk for aspiration pneumonia.
Pathological gambling and other impulse control disorders: Patients experience increased urges, particularly for gambling, and the inability to control these urges while taking Aripiprazole. Other urges, reported, include: increased sexual urges, compulsive shopping, binge or compulsive eating, and other impulsive and compulsive behaviors. It is important for prescribers to ask patients or their caregivers specifically about the development of new or increased gambling urges, sexual urges, compulsive shopping, binge or compulsive eating, or other urges while being treated with Aripiprazole. It should be noted that impulse-control symptoms can be associated with the underlying disorder; however, in some cases, urges were reported to have stopped when the dose was reduced or the medication was discontinued. Impulse control disorders may result in harm to the patient and others if not recognized. Consider dose reduction or stopping the medication if a patient develops such urges while taking Aripiprazole.
Lactase: The tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorptions should not take this medicinal product.
Patients with attention deficit hyperactivity disorder (ADHD) comorbidity: Extreme caution should be taken when these medicinal products are co-administered.
Falls: Aripiprazole may cause somnolence, postural hypotension, motor and sensory instability, which may lead to falls. Caution should be taken when treating patients at higher risk, and a lower starting dose should be considered (e.g. elderly or debilitated patients).
Pregnancy: Patients must be advised to notify their physician if they become pregnant or intend to become pregnant during treatment with Aripiprazole. This medicinal product should not be used in pregnancy unless the expected benefit clearly justifies the potential risk to the fetus.
Newborn infants exposed to antipsychotics (including Aripiprazole) during the third trimester of pregnancy are at risk of adverse reactions including extrapyramidal and/or withdrawal symptoms that may vary in severity and duration following delivery. There have been reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, or feeding disorder. Consequently, newborn infants should be monitored carefully.
Breastfeeding: Aripiprazole is excreted in human breast milk. A decision must be made whether to discontinue breastfeeding or to discontinue/abstain from Aripiprazole therapy taking into account the benefit of breastfeeding for the child and the benefit of therapy for the woman.
Fertility: Aripiprazole did not impair fertility.
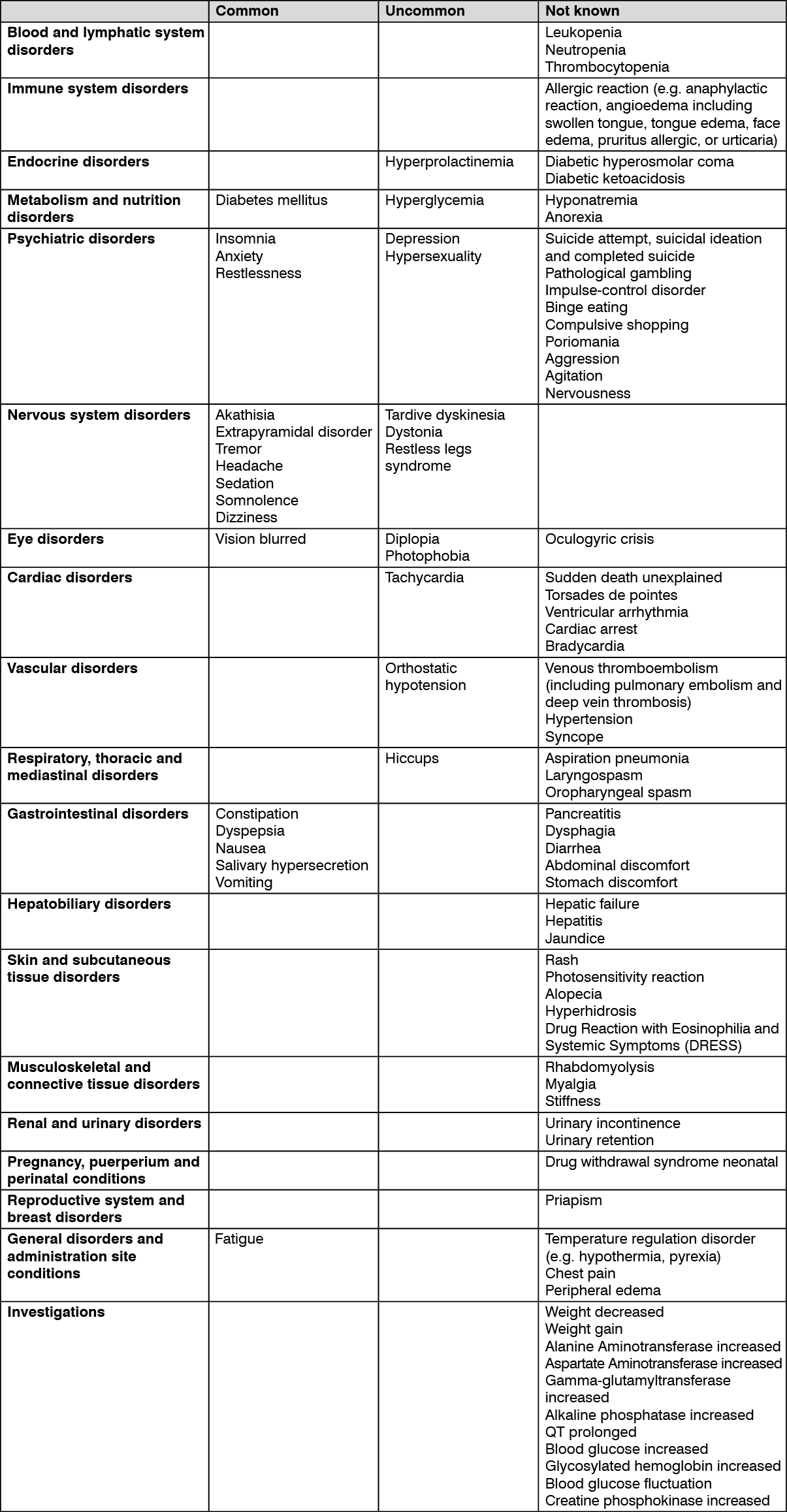
Tabulated list of adverse reactions: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Seek medical attention immediately at the first sign of any adverse reaction.
Due to its α 1-adrenergic receptor antagonism, Aripiprazole has the potential to enhance the effect of certain antihypertensive medicinal products.
Given the primary CNS effects of Aripiprazole, caution should be used when Aripiprazole is administered in combination with alcohol or other CNS medicinal products with overlapping adverse reactions such as sedation.
If Aripiprazole is administered concomitantly with medicinal products known to cause QT prolongation or electrolyte imbalance, caution should be used.
Potential for other medicinal products to affect Aripiprazole: A gastric acid blocker, the H2 antagonist Famotidine, reduces Aripiprazole rate of absorption but this effect is deemed not clinically relevant. Aripiprazole is metabolized by multiple pathways involving the CYP2D6 and CYP3A4 enzymes but not CYP1A enzymes. Thus, no dosage adjustment is required for smokers.
Quinidine and other CYP2D6 inhibitors: Aripiprazole dose should be reduced to approximately one-half of its prescribed dose when concomitant administration of Aripiprazole with Quinidine occurs. Other strong inhibitors of CYP2D6, such as Fluoxetine and Paroxetine, may be expected to have similar effects and similar dose reductions should therefore be applied.
Ketoconazole and other CYP3A4 inhibitors: In CYP2D6 poor metabolizers, concomitant use of strong inhibitors of CYP3A4 may result in higher plasma concentrations of Aripiprazole compared to that in CYP2D6 extensive metabolizers. When considering concomitant administration of Ketoconazole or other strong CYP3A4 inhibitors with Aripiprazole, potential benefits should outweigh the potential risks to the patient. When concomitant administration of Ketoconazole with Aripiprazole occurs, Aripiprazole dose should be reduced to approximately one-half of its prescribed dose. Other strong inhibitors of CYP3A4, such as Itraconazole and HIV protease inhibitors may be expected to have similar effects and similar dose reduction should therefore be applied. Upon discontinuation of the CYP2D6 or CYP3Q4 inhibitor, the dosage of Aripiprazole should be increased to the level prior to the initiation of the concomitant therapy. When weak inhibitors of CYP3A4 (e.g. Diltiazem) or CYP2D6 (e.g. Escitalopram) are used concomitantly with Aripiprazole, modest increases in plasma Aripiprazole concentrations may be expected.
Carbamazepine and other CYP3A4 inducers: Aripiprazole dose should be doubled when concomitant administration of Aripiprazole occurs with Carbamazepine. Concomitant administration of Aripiprazole and other inducers of CYP3A4 (such as Rifampicin, Rifabutin, Phenytoin, Phenobarbital, Primidone, Efavirenz, Nevirapine and St. John's Wort) may be expected to have similar effects and similar dose increases should therefore be applied. Upon discontinuation of strong CYP3A4 inducers, the dosage of Aripiprazole should be reduced to the recommended dose.
Valproate and Lithium: When either Valproate or Lithium was administered concomitantly with Aripiprazole, there was no clinically significant change in Aripiprazole concentrations and therefore no dose adjustment is necessary when either Valproate or Lithium is administered with Aripiprazole.
Potential for Aripiprazole to affect other medicinal products: The 10 mg/day to 30 mg/day doses of Aripiprazole had no significant effect on the metabolism of substrates of CYP2D6 (Dextromethorphan/3-methoxymorphinan ratio), CYP2C9 (Warfarin), CYP2C19 (Omeprazole), and CYP3A4 (Dextromethorphan). Additionally, Aripiprazole and dehydro-aripiprazole did not show potential for altering CYP1A2-mediated metabolism in vitro. Thus, Aripiprazole is unlikely to cause clinically important medicinal product interactions mediated by these enzymes.
When Aripiprazole was administered concomitantly with either Valproate, Lithium or Lamotrigine, there was no clinically important change in Valproate, Lithium or Lamotrigine concentrations.
Serotonin syndrome: Cases of serotonin syndrome have been reported in patients taking Aripiprazole, and possible signs and symptoms for this condition can occur especially in cases of concomitant use with other serotonergic medicinal products, such as selective serotonin reuptake inhibitor/selective serotonin noradrenaline reuptake inhibitor (SSRI/SNRI), or with medicinal products that are known to increase Aripiprazole concentrations.
Store at temperatures not exceeding 30°C.
N05AX12 - aripiprazole ; Belongs to the class of other antipsychotics.
Aripraz 10 FC tab 10 mg
3 × 10's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out