Pharmacotherapeutic group: Antithrombotic agents, direct factor Xa inhibitor.
Pharmacology: Pharmacodynamics: Mechanism of action: Apixaban is a potent, oral, reversible, direct and highly selective active site inhibitor of factor Xa. It does not require antithrombin III for antithrombotic activity. Apixaban inhibits free and clot-bound factor Xa, and prothrombinase activity. Apixaban has no direct effects on platelet aggregation, but indirectly inhibits platelet aggregation induced by thrombin. By inhibiting factor Xa, Apixaban prevents thrombin generation and thrombus development. Preclinical studies of Apixaban in animal models have demonstrated antithrombotic efficacy in the prevention of arterial and venous thrombosis at doses that preserved haemostasis.
Pharmacodynamic effects: The pharmacodynamic effects of Apixaban are reflective of the mechanism of action (FXa inhibition). As a result of FXa inhibition, Apixaban prolongs clotting tests such as prothrombin time (PT), INR and activated partial thromboplastin time (aPTT). Changes observed in these clotting tests at the expected therapeutic dose are small and subject to a high degree of variability. They are not recommended to assess the pharmacodynamic effects of Apixaban. In the thrombin generation assay, Apixaban reduced endogenous thrombin potential, a measure of thrombin generation in human plasma.
Apixaban also demonstrates anti-FXa activity as evident by reduction in Factor Xa enzyme activity in multiple commercial anti-FXa kits, however results differ across kits. Data from clinical studies are only available for the Rotachrom Heparin chromogenic assay. Anti-FXa activity exhibits a close direct linear relationship with Apixaban plasma concentration, reaching maximum values at the time of Apixaban peak plasma concentrations. The relationship between Apixaban plasma concentration and anti-FXa activity is approximately linear over a wide dose range of Apixaban.
The dose- and concentration-related changes observed following Apixaban administration are more pronounced, and less variable, with anti-FXa activity compared with clotting tests.
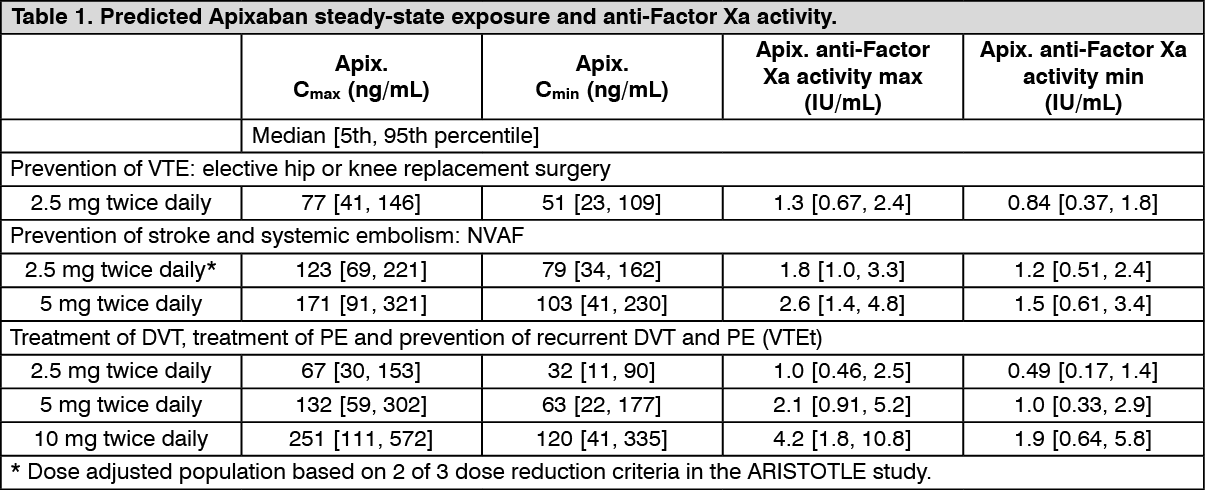
Table 1 as follows shows the predicted steady state exposure and anti-Factor Xa activity for each indication. In patients taking Apixaban for the prevention of VTE following hip or knee replacement surgery, the results demonstrate a less than 1.6-fold fluctuation in peak-to-trough levels. In non-valvular atrial fibrillation patients taking Apixaban for the prevention of stroke and systemic embolism, the results demonstrate a less than 1.7-fold fluctuation in peak-to-trough levels. In patients taking Apixaban for the treatment of DVT and PE or prevention of recurrent DVT and PE, the results demonstrate a less than 2.2-fold fluctuation in peak-to-trough levels. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Although treatment with Apixaban does not require routine monitoring of exposure, a calibrated quantitative anti-Factor Xa assay may be useful in exceptional situations where knowledge of Apixaban exposure may help to inform clinical decisions, e.g., overdose and emergency surgery.
Pharmacokinetics: Absorption: The absolute bioavailability of Apixaban is approximately 50% for doses up to 10 mg. Apixaban is rapidly absorbed with maximum concentrations (C
max) appearing 3 to 4 hours after tablet intake. Intake with food does not affect Apixaban AUC or C
max at the 10 mg dose. Apixaban can be taken with or without food. Apixaban demonstrates linear pharmacokinetics with dose proportional increases in exposure for oral doses up to 10 mg. At doses ≥25 mg, Apixaban displays dissolution limited absorption with decreased bioavailability. Apixaban exposure parameters exhibit low to moderate variability reflected by a within-subject and inter-subject variability of ~20% CV and ~30% CV, respectively.
Following oral administration of 10 mg of Apixaban as 2 crushed 5 mg tablets suspended in 30 mL of water, exposure was comparable to exposure after oral administration of 2 intact 5 mg tablets. Following oral administration of 10 mg of Apixaban as 2 crushed 5 mg tablets mixed with 30 g of applesauce, the C
max and AUC were 21% and 16% lower, respectively, when compared to administration of 2 intact 5 mg tablets. Following administration of a crushed 5 mg Apixaban tablet suspended in 60 mL of D5W and delivered via a nasogastric tube, exposure was similar to exposure seen in other clinical trials involving healthy subjects receiving a single oral 5 mg Apixaban tablet dose.
Distribution: Plasma protein binding in humans is approximately 87%. The volume of distribution (Vss) is approximately 21 liters.
Metabolism and Elimination: Apixaban has multiple routes of elimination. Of the administered Apixaban dose in humans, approximately 25% was recovered as metabolites, with the majority recovered in feces. Renal excretion of Apixaban accounts for approximately 27% of total clearance. Additional contributions from biliary and direct intestinal excretion were observed in clinical and nonclinical studies, respectively.
Apixaban has a total clearance of about 3.3 L/h and a half-life of approximately 12 hours. O-demethylation and hydroxylation at the 3-oxopiperidinyl moiety are the major sites of biotransformation. Apixaban is metabolized mainly via CYP3A4/5 with minor contributions from CYP1A2, 2C8, 2C9, 2C19, and 2J2. Unchanged Apixaban is the major drug-related component in human plasma with no active circulating metabolites present. Apixaban is a substrate of transport proteins, P-gp and breast cancer resistance protein (BCRP).
Renal Impairment: There was no impact of impaired renal function on peak concentration of Apixaban. There was an increase in Apixaban exposure correlated to decrease in renal function, as assessed via measured creatinine clearance. In individuals with mild (creatinine clearance 51-80 mL/min), moderate (creatinine clearance 30-50 mL/min) and severe (creatinine clearance 15-29 mL/min) renal impairment, Apixaban plasma concentrations (AUC) were increased 16, 29, and 44% respectively, compared to individuals with normal creatinine clearance. Renal impairment had no evident effect on the relationship between Apixaban plasma concentration and anti-FXa activity. No dose adjustment is necessary in patients with mild, moderate or severe renal impairment except as described in Dosage & Administration.
In subjects with end-stage renal disease (ESRD), the AUC of Apixaban was increased by 36% when a single dose of Apixaban 5 mg was administered immediately after hemodialysis, compared to that seen in subjects with normal renal function. Hemodialysis, started two hours after administration of a single dose of Apixaban 5 mg, decreased Apixaban AUC by 14% in these ESRD subjects, corresponding to an Apixaban dialysis clearance of 18 mL/min.
Hepatic Impairment: Apixaban has not been studied in patients with severe hepatic impairment or active hepatobiliary disease. Apixaban is not recommended in patients with severe hepatic impairment (see Precautions).
Elderly: Elderly patients (above 65 years) exhibited higher plasma concentrations than younger patients, with mean AUC values being approximately 32% higher. No dose adjustment is required, except as described in Recommended Dosage: Prevention of stroke and systemic embolism in patients with AF: NVAF under Dosage & Administration.
Gender: Exposure to Apixaban was approximately 18% higher in females than in males. No dose adjustment is required.
Ethnic Origin and Race: The results across phase 1 studies showed no discernible difference in Apixaban pharmacokinetics between White/Caucasian, Asian and Black/African American subjects. Findings from a population pharmacokinetic analysis in patients who received Apixaban following elective hip or knee replacement surgery were generally consistent with the phase 1 results. No dose adjustment is required.
Body Weight: Compared to Apixaban exposure in subjects with body weight of 65 to 85 kg, body weight >120 kg was associated with approximately 30% lower exposure and body weight <50 kg was associated with approximately 30% higher exposure. No dose adjustment is required, except as described in Recommended Dosage: Prevention of stroke and systemic embolism in patients with AF: NVAF under Dosage & Administration.
Pharmacokinetic/Pharmacodynamic Relationship: The pharmacokinetic/pharmacodynamic (PK/PD) relationship between Apixaban plasma concentration and several PD endpoints (anti-FXa activity, INR, PT, aPTT) has been evaluated after administration of a wide range of doses (0.5-50 mg). The relationship between Apixaban plasma concentration and anti-FXa activity was best described by a linear model. The PK/PD relationship observed in patients who received Apixaban in Phase 2 or Phase 3 clinical trials was consistent with that established in healthy subjects.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out