



 Sign Out
Sign Out


Study 201 (ALTA): A randomized, open-label, multicenter trial in patients treated with brigatinib with ALK+ NSCLC who previously progressed on crizotinib. Patients were randomized in a 1:1 ratio to receive brigatinib either 90 mg once daily continuously (90 mg regimen, n=112) or 180 mg once daily with a 7-day lead-in at 90 mg once daily (180 mg regimen, n=110).
Study 101: An open-label multicenter phase 1/2 dose escalation/expansion trial in patients with advanced malignancies.
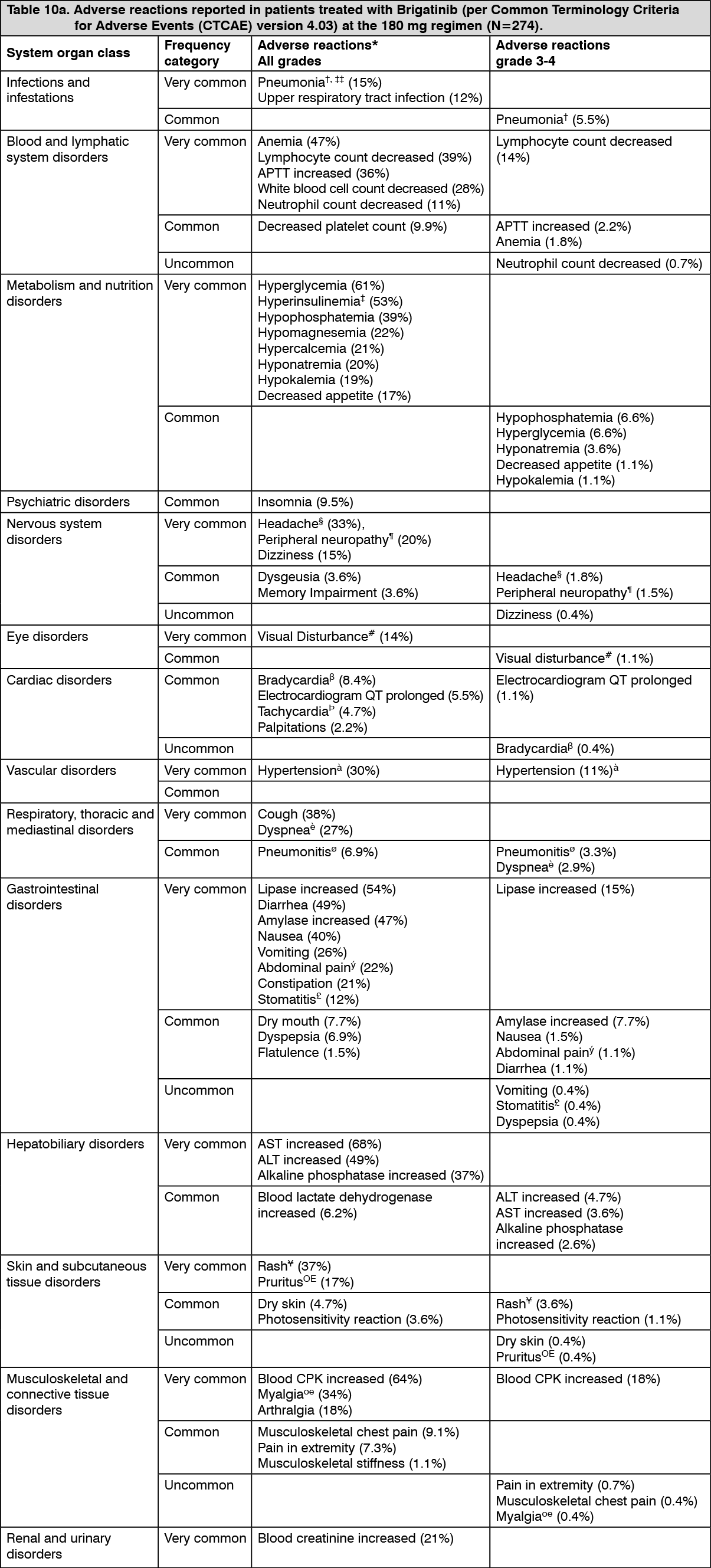
The most common adverse reactions reported in patients (≥25%) treated with brigatinib at the 180 mg regimen were increased AST (68%), increased CPK (64%), hyperglycemia (61%), increased lipase (54%), hyperinsulinemia (53%), diarrhea (49%), increased ALT (49%), increased amylase (47%), anemia (47%), nausea (40%), fatigue (40%), hypophosphatemia (39%), decreased lymphocyte count (39%), cough (38%), rash (37%), increased alkaline phosphatase (37%), increased APTT (36%), myalgia (34%), headache (33%), hypertension (30%), white blood count decreased (28%), dyspnea (27%), and vomiting (26%).
The most common serious adverse reactions reported in 2% or more of patients at the 180 mg regimen other than events related to neoplasm progression included pneumonia (6.9%), pneumonitis (5.5%), dyspnea (2.9%) and pyrexia (2.2%).
Treatment-emergent adverse events (TEAEs) that led to discontinuation of brigatinib occurred in 12% of patients receiving the 180 mg regimen. The most common TEAEs (occurring in ≥2 patients receiving the 180 mg regimen) other than events related to neoplasm progression that led to brigatinib discontinuation were pneumonitis 3.3%, pneumonia 1.8% and bradycardia 0.7%.
TEAEs that led to dose reduction occurred in 32.8% of patients receiving the 180 mg regimen. The TEAEs leading to dose reduction that occurred in ≥2% of patients receiving the 180 mg regimen were blood CPK increased 10.2%, lipase increased 4.7%, rash 3.3%, and amylase increased 2.9%.
Adverse reactions reported in Table 10 are listed by system organ class, preferred term and frequency. The following convention is used for the classification of the frequency of an adverse drug reaction (ADR) and is based on the Council for International Organizations of Medical Sciences (CIOMS) guidelines: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data). (See Tables 10a and 10b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image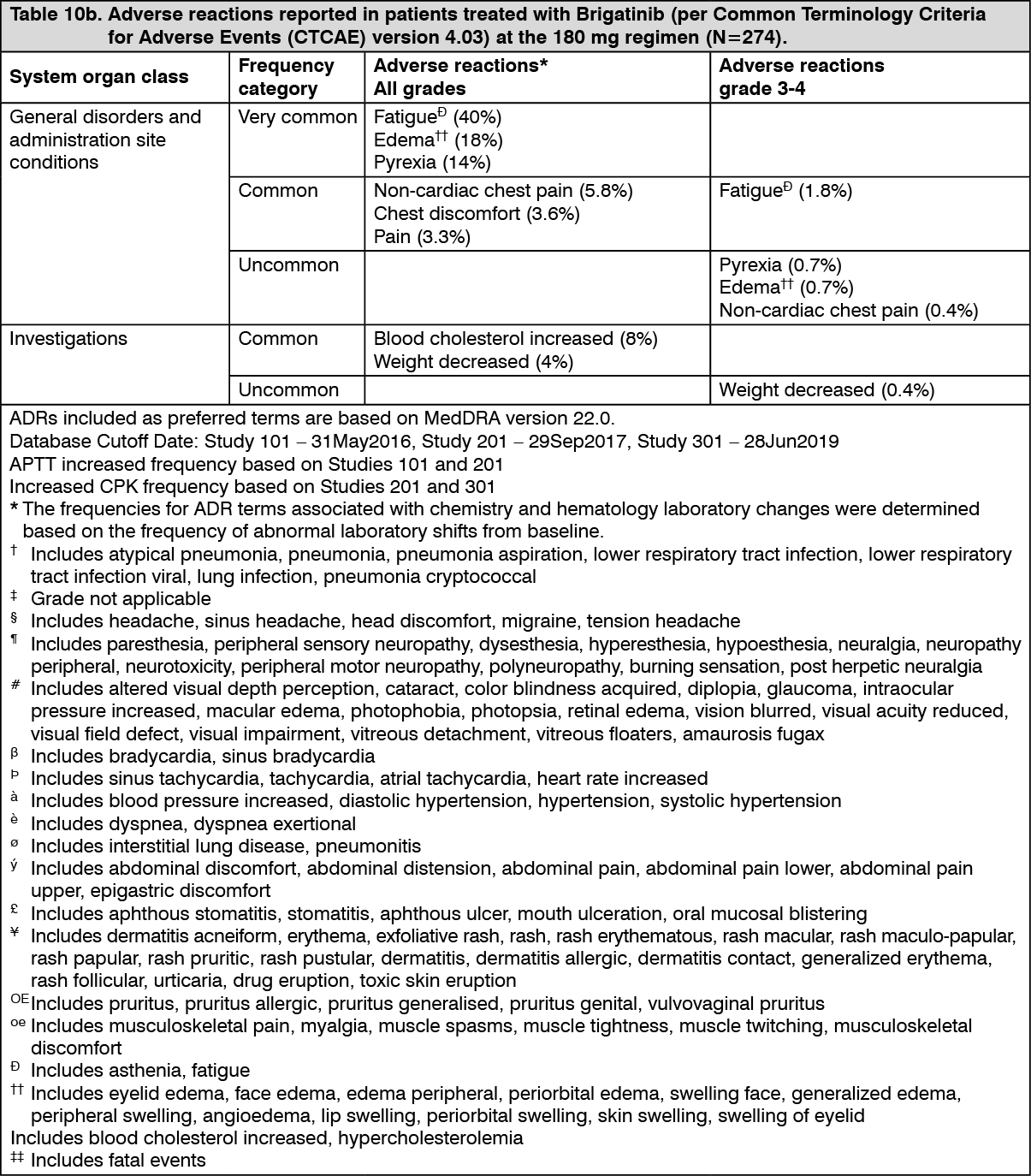 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePulmonary Adverse Reactions: In ALTA 1L, 2.9% of patients experienced any grade ILD/pneumonitis early in treatment (within 8 days), with Grade 3-4 ILD/pneumonitis in 2.2% of patients. There were no fatal ILD/pneumonitis. Additionally, 3.7% of patients experienced pneumonitis later in treatment.
In ALTA, pulmonary adverse reactions of any grade, including ILD/pneumonitis, pneumonia and dyspnea, early in treatment (within 9 days, median onset: 2 days), were experienced in 6.4% of patients; 2.7% of patients had Grade 3-4 pulmonary adverse reactions and 1 patient (0.5%) had fatal pneumonia. Following Grade 1-2 pulmonary adverse reactions, treatment with brigatinib was either interrupted and then restarted or the dose was reduced. Additionally, 2.3% of patients experienced pneumonitis later in treatment, with 2 patients having Grade 3 pneumonitis (see Dosage & Administration and Precautions).
Hypertension: Hypertension was reported in 30% of patients treated with brigatinib at the 180 mg regimen with 11% having Grade 3 hypertension. Dose reduction for hypertension occurred in 1.5% of patients at the 180 mg regimen (see Dosage & Administration and Precautions).
Bradycardia: Bradycardia was reported in 8.4% of patients treated with brigatinib at the 180 mg regimen.
Heart rates of less than 50 beats per minute (bpm) were reported in 8.4% of patients at the 180 mg regimen (see Dosage & Administration and Precautions).
Visual Disturbance: Visual disturbance adverse reactions were reported in 14% of patients treated with brigatinib at the 180 mg regimen. Of these, three grade 3 adverse reactions (1.1%) including macular edema (1) and cataract (2) were reported.
Dose reduction for visual disturbance occurred in two patients (0.7%) at the 180 mg regimen (see Dosage & Administration and Precautions).
Creatine Phosphokinase (CPK) Elevation: In ALTA 1L and ALTA, elevations of creatine phosphokinase (CPK) were reported in 64% of patients treated with brigatinib at the 180 mg regimen. The incidence of Grade 3-4 elevations of CPK was 18%. The median time to onset for CPK elevations was 28 days.
Dose reduction for CPK elevation occurred in 10% patients at the 180 mg regimen (see Dosage & Administration and Precautions).
Elevations of Pancreatic Enzymes: Elevations of amylase and lipase were reported in 47% and 54% of patients treated with brigatinib, respectively at the 180 mg regimen. For elevations to Grades 3-4, the incidences for amylase and lipase were 7.7% and 15%, respectively. The median time to onset for amylase elevations and lipase elevations was 16 days and 29 days, respectively.
Dose reduction for elevation of lipase and amylase occurred in 4.7% and 2.9% of patients, respectively at the 180 mg regimen (see Dosage & Administration and Precautions).
Elevation of Hepatic Enzymes: Elevations of ALT and AST were reported in 49% and 68% of patients treated with brigatinib, respectively at the 180 mg regimen. For elevations to Grades 3-4, the incidences for ALT and AST were 4.7% and 3.6%, respectively. The median time to onset for ALT elevations and AST elevations was 42 days and 28 days, respectively.
Dose reduction for elevation of ALT and AST occurred in 0.7% and 1.1% of patients, respectively at the 180 mg regimen (see Dosage & Administration and Precautions).
Hyperglycemia: Sixty-one percent of patients experienced hyperglycemia. Grade 3 hyperglycemia occurred in 6.6% of patients (see Dosage & Administration and Precautions).
No patients had dose reductions due to hyperglycemia.
Photosensitivity: Photosensitivity was reported in 3.6% patients treated with brigatinib at the 180 mg regimen. Grade 3-4 photosensitivity occurred in 1.1% of patients.
Dose reduction for photosensitivity occurred in two patients (0.7%) at the 180 mg regimen (see Dosage & Administration and Precautions).
Postmarketing: Not applicable.
View ADR Reporting Link