



 Sign Out
Sign Out
In addition HPVL1 mRNA and HPV DNA are significantly decreased following treatment. However, the clinical relevance of these findings is unknown.
Superficial Basal Cell Carcinoma: The mechanism of action of Imiquimod (Aldara) Cream in treating superficial basal cell carcinoma (sBCC) lesions is unknown. An open label study in 6 subjects with sBCC suggests that treatment with Imiquimod (Aldara) Cream may increase the infiltration of lymphocytes, dendritic cells and macrophages into the tumor lesion; however, the clinical significance of these findings is unknown.
Pharmacokinetics: Systemic absorption of imiquimod was observed across the affected skin of 12 patients with genital/perianal warts, with an average dose of 4.6 mg. Mean peak drug concentration of approximately 0.4 ng/mL was seen during study. Mean urinary recoveries of imiquimod and metabolites combined over the whole course of treatment, expressed aspercent of the estimated applied dose, were 0.11 and 2.41% in the males and females, respectively. Systemic absorption of imiquimod across the affected skin of 58 patients with actinic keratosis was observed with a dosing frequency of 3 applications per week for 16 weeks. Mean peak serum drug concentrations at the end of week 16 were approximately 0.1, 0.2, and 3.5 ng/mL for the applications to the face (12.5 mg imiquimod, 1 single-use sachet), scalp (25 mg, 2 sachets) and hands/arms (75 mg, 6 sachets), respectively. (See Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe application surface area was not controlled when more than one sachet was used. Dose proportionality was not observed.
However it appears that systemic exposure may be more dependent on surface area of application than amount of applied dose. The apparent half-life was approximately 10 times greater with topical dosing than the 2 hour apparent half-life seen following subcutaneous dosing, suggesting prolonged retention of drug in the skin. Mean urinary recoveries of imiquimod and metabolites combined were 0.08 and 0.15% of the applied dose in the group using 75 mg (6 sachets) for males and females, respectively following 3 applications per week for 16 weeks.
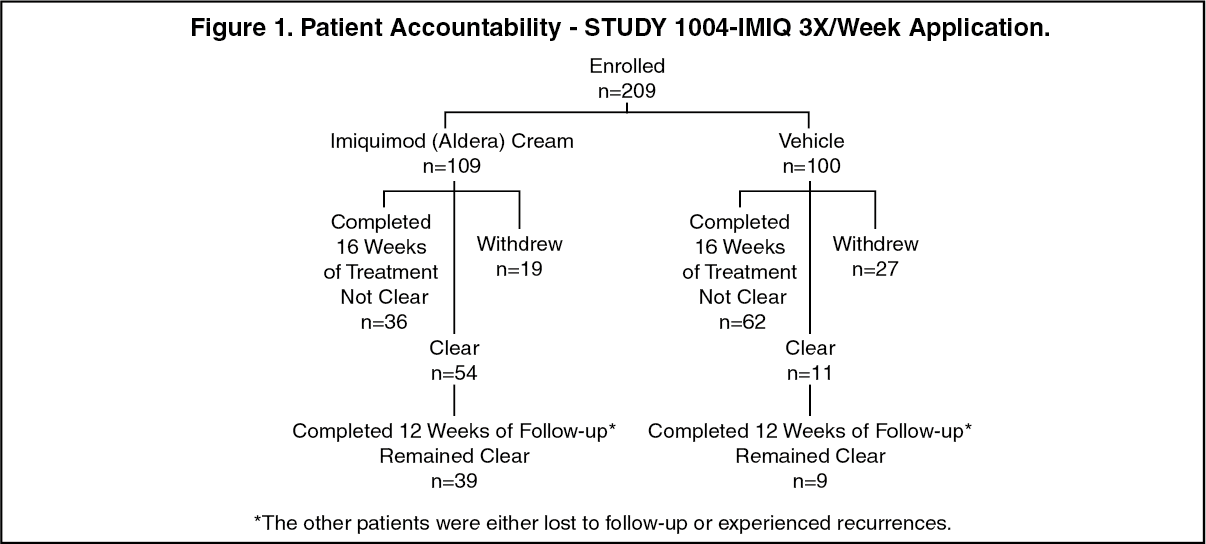
Clinical Studies: External Genital Warts: In a double-blind, placebo-controlled clinical study, 209 otherwise healthy patients ≥18 years with genital/perianal warts were treated with Imiquimod (Aldara) Cream or vehicle control 3X/week for a maximum of 16 weeks. The median baseline warts area was 69 mm2 (range 8-5525 mm2). Patient accountability is shown in Figure 1. (See Figure 1.)
 Click on icon to see table/diagram/image
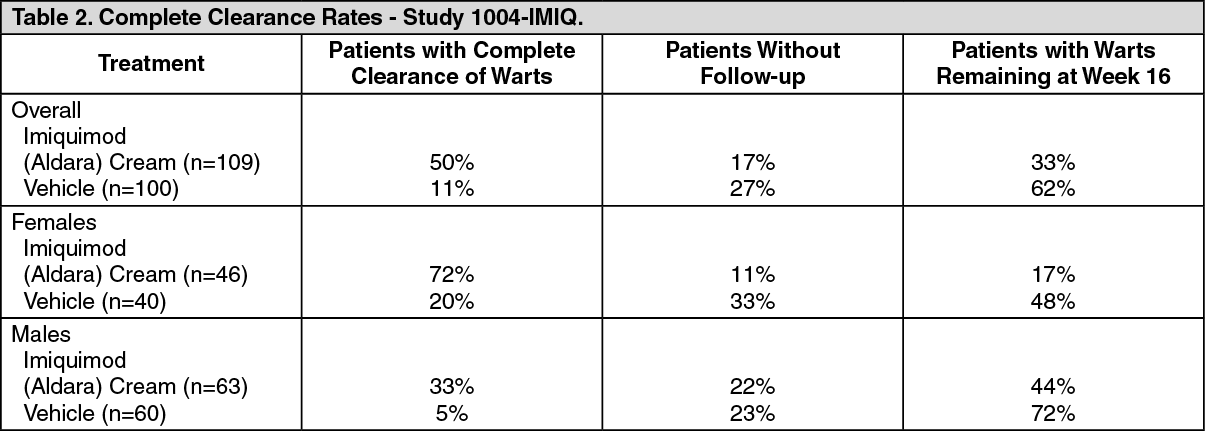
Click on icon to see table/diagram/imageData on complete clearance are listed in Table 2. The median time to complete wart clearance was 10 weeks. (See Table 2.)
 Click on icon to see table/diagram/image
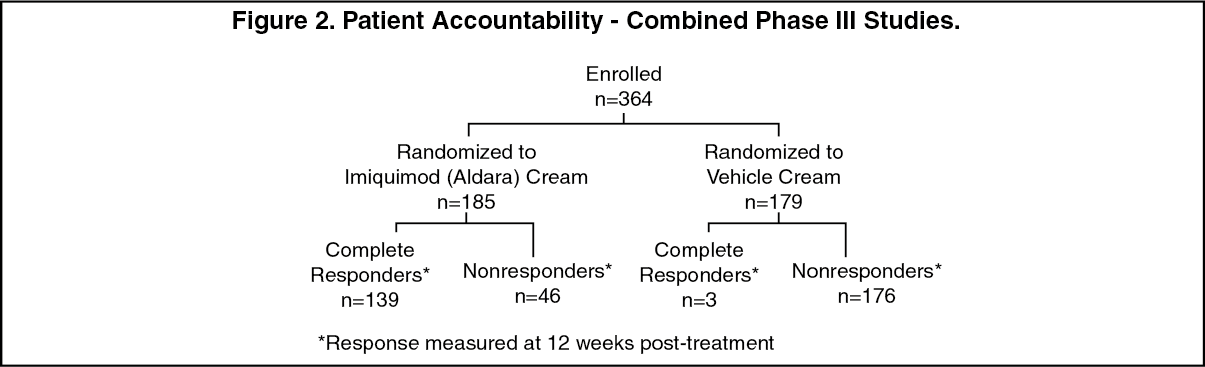
Click on icon to see table/diagram/imageSuperficial Basal Cell Carcinoma: In two double-blind, vehicle-controlled clinical studies, 364 patients with primary superficial basal cell carcinoma (sBCC) were treated with Imiquimod (Aldara) Cream or vehicle cream 5X/week for 6 weeks. Patients with one biopsy-confirmed sBCC tumor were enrolled and randomized in a 1:1 ratio to active or vehicle treatment. Target tumors were to have a minimum area of 0.5 cm2 and a maximum diameter of 2.0 cm (4.0 cm2). Target tumors were not to be located within 1.0 cm of the hairline, eyes, nose, mouth, ears, on the anogenital area or on the hands or feet, or have any atypical features. On a scheduled dosing day, the study cream was applied to the target tumor and approximately 1 cm (about 1/3 inch) beyond the target tumor prior to normal sleeping hours; 5X/week dosing was continued for a total of 6 weeks. Twelve weeks after the last scheduled application of study cream, the target tumor area was clinically assessed. The entire target tumor was then excised and examined histologically for the presence of tumor. The primary efficacy variable was the complete response rate defined as the proportion of patients with clinical(visual) and histological clearance of the sBCC lesion at 12 weeks post-treatment. The population ranged from 31-89 years of age (median 60 years) and 65% had Fitzpatrick skin type I or II.
Patients outcome are shown in the figure as follows. (See Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOf Imiquimod (Aldara)-treated patients 6% (11/178) who both clinical and histological assessments post-treatment and appeared to be clinically clear in studies C and D had evidence of tumor on excision of the clinically clear treatment area. Data on composite clearance (defined as both clinical and histological clearance) are shown in the table as follows. (See Table 3.)
 Click on icon to see table/diagram/image
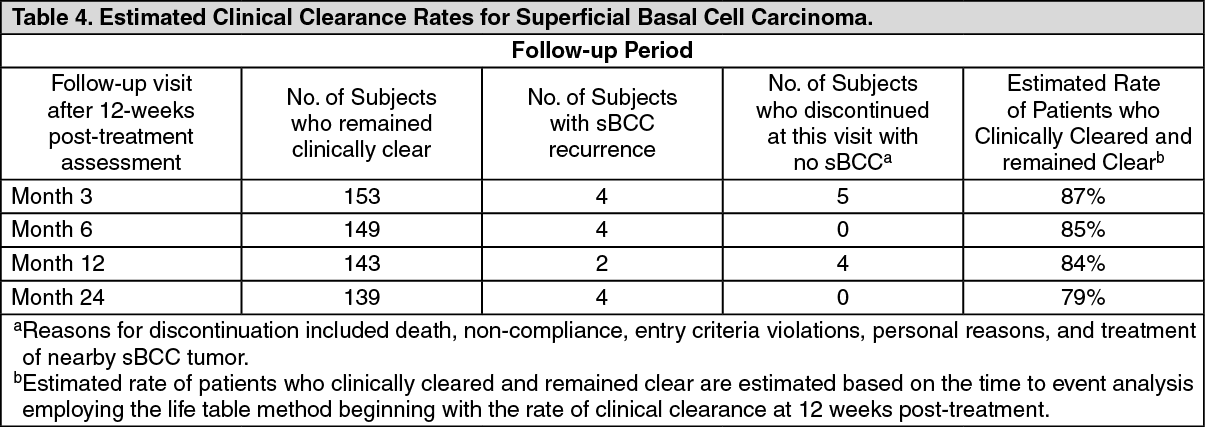
Click on icon to see table/diagram/imageAn open-label 5-year study (study E) is ongoing to assess the recurrence of sBCC treated with Imiquimod (Aldara) Cream applied once daily 5 days per week for 6 weeks. Target tumor inclusion criteria were the same as for studies C and D as described in the previous text. At 12-week post-treatment, patients were clinically (no histological assessment evaluated for evidence of persistent sBCC. Subjects with no clinical evidence of BCC entered the long-term follow-up period. At the 12-week post-treatment assessment 163/182 (90%) of the subjects enrolled had no clinical evidence of sBCC at their target site and 162 subjects entered the long-term follow-up period for up to 5 years. Two years (24 months) follow-up data are available from this study and are presented in the following table: (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image